Educational example only - This is a fictitious report created to help you understand how I read and interpret a Penile Doppler. No real patient data is shown.
Penile Colour Doppler Ultrasound
Mr Giangiacomo Ollandini · Consultant Urological Surgeon
Patient Ref: EXAMPLE-001 · Date: [Fictitious]
Chelsea & Westminster Hospital
False venous leak resolved with adrenergic blockade
Clinical background
32-year-old man referred with 18-month history of erectile difficulty. Reports erections adequate during masturbation but inconsistent with partner. Morning erections present but perceived as reduced. No significant cardiovascular risk factors. BMI 24. Non-smoker. No regular medications. Referred by GP after trial of sildenafil 50mg with partial response.
Technique
Pharmacostimulation: Alprostadil 10 mcg intracavernosal injection (T=0). B-mode and colour Doppler assessment of both cavernosal arteries at serial intervals. Patient counselled throughout. Privacy maintained.
B-mode findings
Corpora cavernosa symmetrical with homogeneous echotexture bilaterally. No plaque, fibrosis, or calcification identified. Tunica albuginea intact. Both cavernosal arteries visualised - right 0.8 mm, left 0.7 mm at baseline. Regular walls, no stenosis.
Haemodynamic findings - Test 1 (Alprostadil only)
| Time | Side | PSV (cm/s) | EDV (cm/s) | RI | Tumescence | HR |
|---|---|---|---|---|---|---|
| T+5 min | R | 48 | 14 | 0.71 | Partial | 106 |
| T+5 min | L | 45 | 13 | 0.71 | Partial | 106 |
| T+10 min | R | 59 | 12 | 0.80 | Partial | 102 |
| T+10 min | L | 55 | 12 | 0.78 | Partial | 102 |
| T+15 min | R | 56 | 11 | 0.80 | Partial+ | 100 |
| T+15 min | L | 52 | 11 | 0.79 | Partial+ | 100 |
| T+20 min | R | 52 | 11 | 0.79 | Partial+ | 98 |
| T+20 min | L | 50 | 10 | 0.80 | Partial+ | 98 |
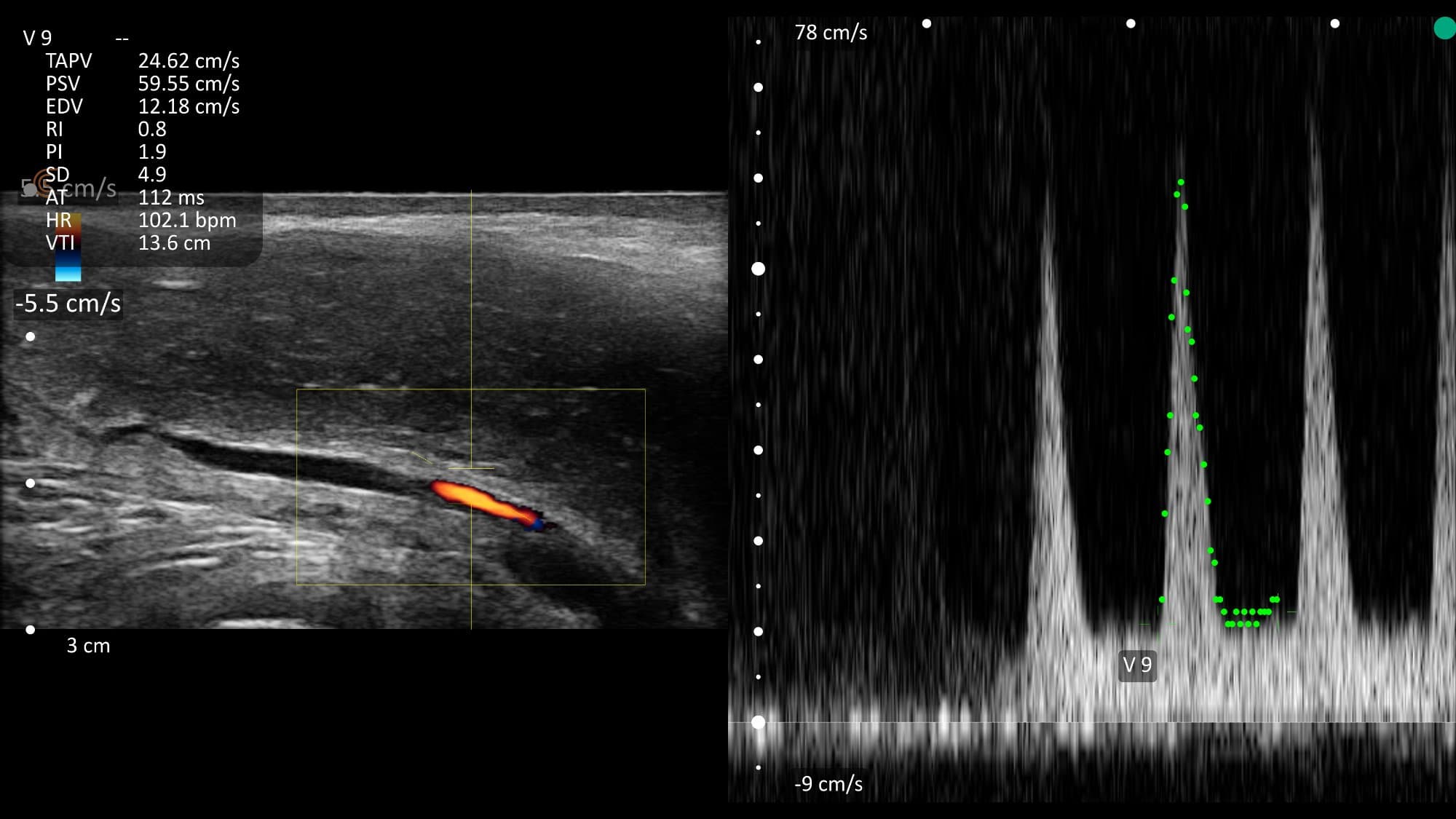
Haemodynamic observations - Test 1: Bilateral PSV consistently above 45 cm/s, peaking at 59 cm/s - arterial inflow is adequate. However, end-diastolic velocity remains elevated throughout (10-14 cm/s), and the patient did not achieve full rigidity. RI remains below 0.90 at all time points.
Heart rate remained between 98-106 bpm throughout the study. Patient appeared tense despite verbal reassurance.
Pattern: This haemodynamic profile is consistent with either corporoveno-occlusive dysfunction or sympathetic override in an anxious patient. A repeat study with phentolamine was offered to differentiate.
Haemodynamic findings - Test 2 (Alprostadil + Phentolamine)
Repeat study performed on a separate date. Same protocol with addition of phentolamine 1 mg to the injection mix.
| Time | Side | PSV (cm/s) | EDV (cm/s) | RI | Tumescence | HR |
|---|---|---|---|---|---|---|
| T+5 min | R | 56 | 3 | 0.95 | Full | 78 |
| T+5 min | L | 52 | 2 | 0.96 | Full | 78 |
| T+10 min | R | 55 | -5 | 1.09 | Full rigid | 76 |
| T+10 min | L | 52 | -6 | 1.12 | Full rigid | 76 |
| T+15 min | R | 53 | -9 | 1.20 | Full rigid | 75 |
| T+15 min | L | 50 | -10 | 1.20 | Full rigid | 75 |
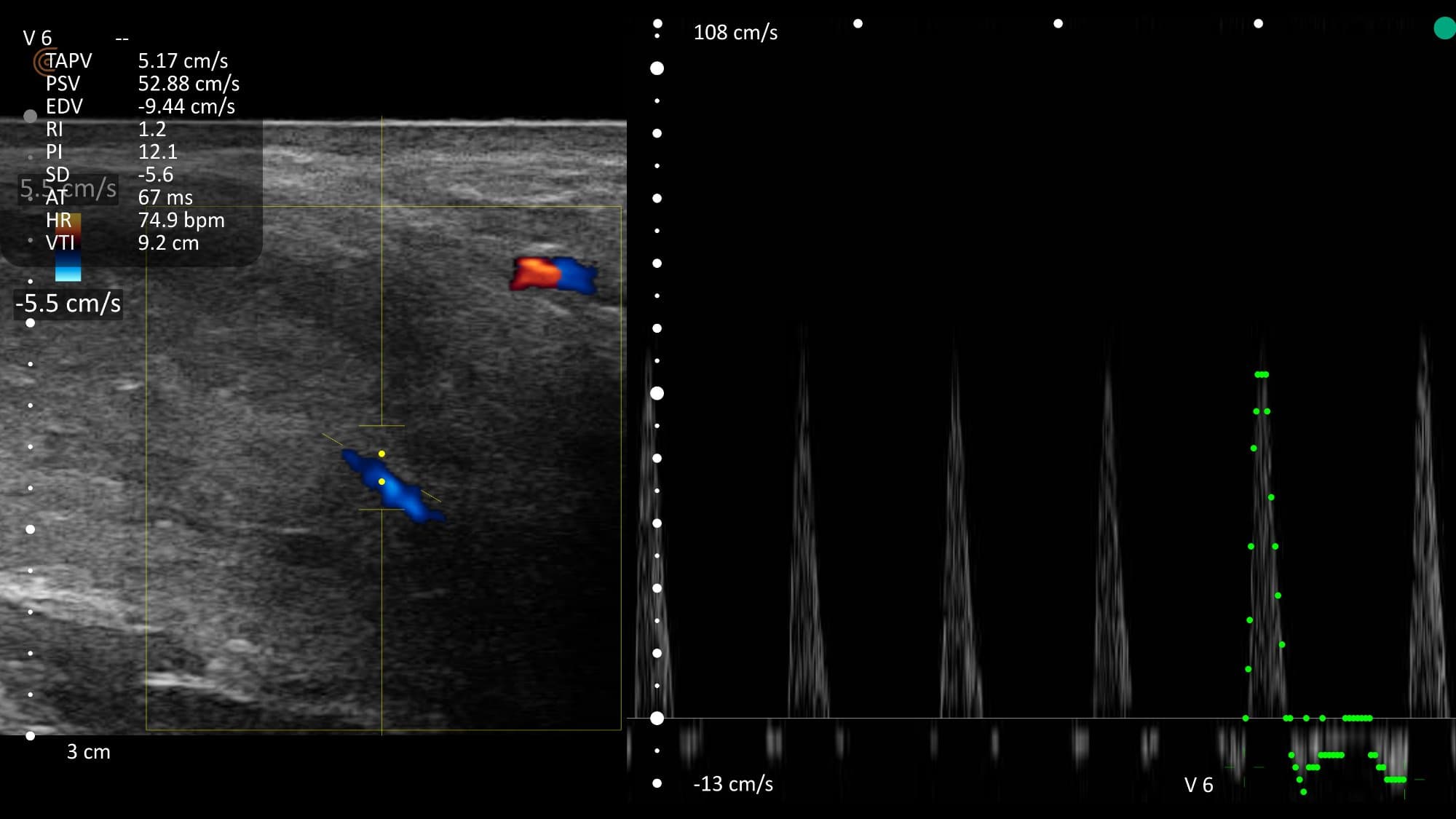
Haemodynamic observations - Test 2: With phentolamine blocking adrenergic override, EDV dropped from 10-14 cm/s to 2-3 cm/s within 5 minutes, and became strongly negative (reversed diastolic flow reaching -9 to -10 cm/s) by T+15 - indicating excellent veno-occlusive function.
Full rigid erection achieved. RI exceeded 0.95 bilaterally. Heart rate settled to 75 bpm.
Conclusion: The apparent veno-occlusive dysfunction seen in Test 1 is not confirmed on repeat testing with adrenergic blockade. The haemodynamic pattern is consistent with sympathetic override (anxiety-mediated) rather than structural venous leak. Arterial inflow is normal. Veno-occlusive mechanism is intact.
The key difference: Same scan, same numbers on the screen - but one is anxiety forcing the gates open (fixable without surgery), and the other is gates with structural holes (requires a different conversation). This is why protocol, context, and clinical judgment matter more than any single number.
Powered by GGO Med