


- Performed by a consultant urologist (never outsourced)
- Clear medical indications — and honest advice when surgery isn’t needed
- Transparent self-pay pricing (insured patients welcome too) and structured recovery plan
Ready to discover your options?
Not everyone who enquires needs circumcision — we’ll discuss options first.
What actually happens if you choose surgery
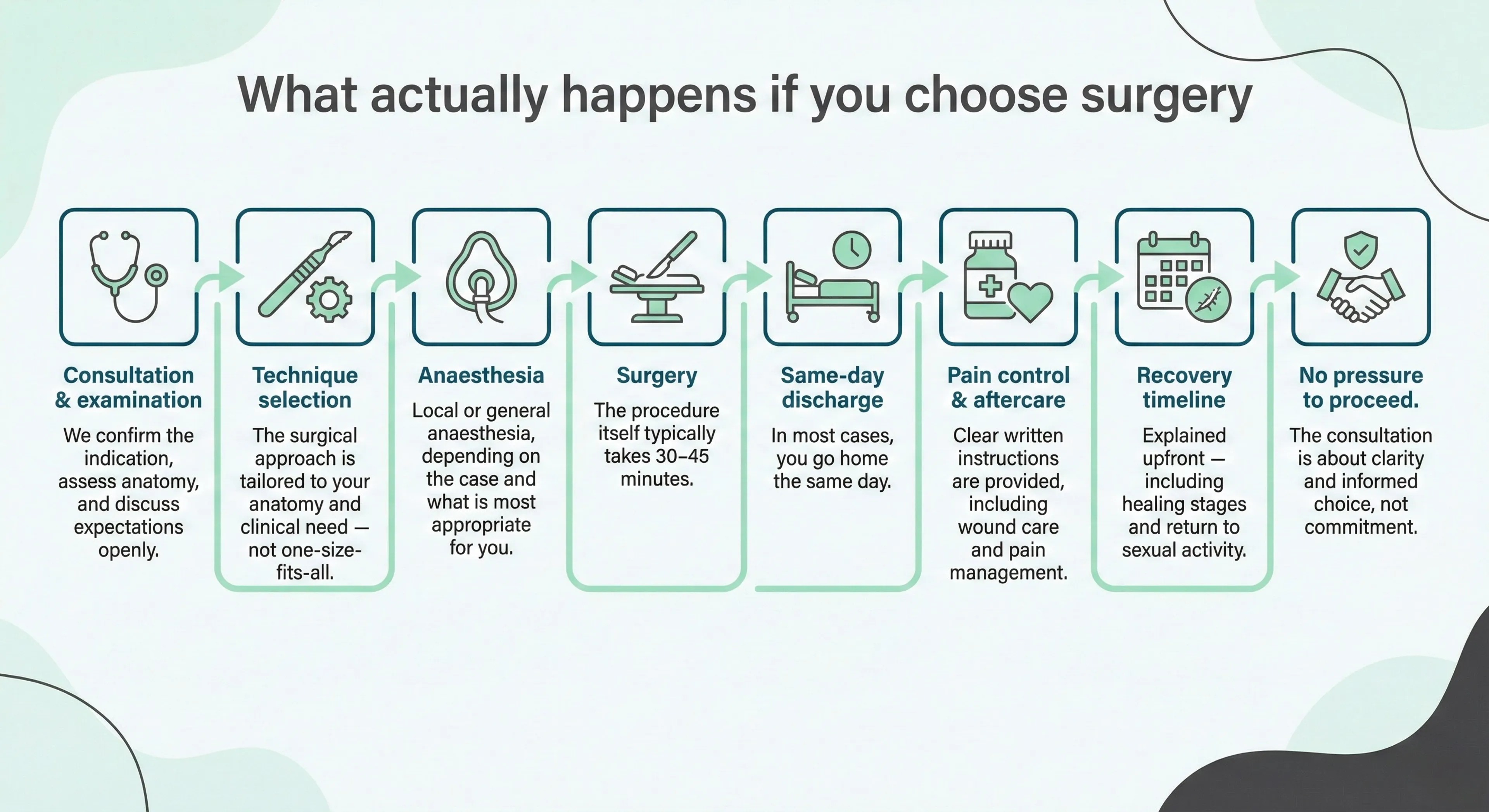
The consultation confirms the indication, selects the right technique, covers anaesthesia, and sets clear expectations for recovery and return to sexual activity.
There is no pressure to proceed — the goal is clarity, not commitment.
You're considering circumcision as an adult. Maybe you've been told you need it. Maybe you've decided you want it. Either way, you probably have questions you're not sure how to ask.
This page tells you exactly what happens — the procedure, the recovery, the risks, and yes, the cost. No vague reassurances. No dodging the uncomfortable bits.
Is circumcision right for me?
Why men have circumcision
Some men need it. Some men choose it. Both are valid reasons.
Medical reasons:
- Phimosis — foreskin too tight to retract, causing problems with hygiene, sex, or urination
- BXO (balanitis xerotica obliterans) — a skin condition that scars the foreskin and won't resolve without surgery
- Recurrent balanitis — repeated infections under the foreskin that don't respond to other treatment
- Paraphimosis — foreskin stuck behind the glans (this is usually an emergency, but circumcision prevents recurrence)
Personal reasons:
- Preference — aesthetic, sexual, or practical
- Religious or cultural practice
- Partner preference
- Hygiene in certain conditions (e.g., limited mobility, catheter use)
Circumcision may not be the best first step if your foreskin is fully retractable and symptoms are mild, or if there hasn’t been a proper discussion of conservative options.
What I don’t provide on this page:
I focus here on adult medical/functional circumcision. If you’re looking for childhood or religious circumcision pathways, this page won’t be the right fit.
Loading decision aid…
Key Points at a Glance
- Circumcision is the complete surgical removal of the foreskin—often the most definitive surgical option for foreskin problems
- Adult circumcision is common and routine—this is not a procedure reserved for children
- Phimosis can be congenital (present from birth) or acquired (developing later in life)—the distinction matters for treatment
- Post-operative hypersensitivity is normal and expected, especially in men with lifelong tight phimosis
- For some men—especially with long-standing tight phimosis—sensory adaptation can take a few months (often around 3–6)
- Circumcision does not affect sperm production or fertility. It does change the mechanics and the 'feel' of sex for many men, and it can take time to settle—especially in the first few months
Quick understanding
If you're considering circumcision, it's usually because your foreskin is causing symptoms — tightness, pain, infections, or hygiene problems — or because you're choosing it for personal, cultural, or religious reasons.
Adult circumcision is common. Much of what to expect centres on recovery and sensitivity changes — especially if your glans has been covered your whole life.
Expand the sections below for full detail: anatomy, treatment alternatives, the step-by-step procedure, and how hypersensitivity settles over time.

Why Are You Considering Circumcision?
If you're reading this, you may be experiencing symptoms that are affecting your quality of life—perhaps a tight foreskin causing discomfort, recurrent infections, pain during intimacy, or concerns about a skin condition. You might also be considering circumcision for personal, cultural, or religious reasons.
Whatever brings you here, I want you to know that you're not alone. In my practice, I see men of all ages—from their twenties to their eighties—seeking help with foreskin-related concerns. Many have delayed seeking advice for years, sometimes decades, due to embarrassment or uncertainty. Some have lived with a tight foreskin their entire lives, assuming it was normal or that nothing could be done.
I understand how personal this is. The decision to undergo circumcision is significant, and my role is to provide you with comprehensive, honest information so you can make the choice that's right for you. This guide aims to answer your questions thoroughly, including topics that are often overlooked—such as what to expect from the recovery process, particularly regarding sensitivity changes.
Adult circumcision
Circumcision is not unusual or reserved for children. Men of all ages have it done, often after living with symptoms for years.
There isn’t a fixed age limit — what matters is your overall health and whether surgery is appropriate for your situation.
Watch: Adult Circumcision Explained
A brief overview of why adult circumcision is more common than you might think — and why it's never too late to seek treatment.
Adult Circumcision: what you need to know about it.
Understanding circumcision
Circumcision removes the foreskin, leaving the glans permanently exposed. The foreskin is a real anatomical structure — not "spare skin" — with inner and outer layers and specialised tissue.
Expand for the core explanation, then expand again for detailed anatomy.
Understanding Circumcision
Circumcision is a surgical procedure that involves the complete removal of the foreskin—the fold of skin that covers the head (glans) of the penis. After circumcision, the glans remains permanently exposed.
The foreskin is a double-layered structure that, in its natural state, retracts during erection and returns to cover the glans when flaccid. It contains nerve endings, blood vessels, and specialised tissue. When the foreskin causes ongoing problems, or when an adult makes an informed choice to proceed, circumcision is a definitive surgical option.
Anatomy of the Foreskin (Prepuce)
The foreskin is a complex structure with several distinct anatomical components:
Outer foreskin: This is continuous with the skin of the penile shaft. It has a similar structure to normal skin, with keratinised epithelium that provides protection.
Inner foreskin: The mucosal surface that lies in contact with the glans. This tissue is thinner, more delicate, and contains a higher density of nerve endings than the outer surface. It produces secretions that help maintain moisture and reduce friction.
Preputial ring: The narrowest part of the foreskin opening. In phimosis, it is this ring that is too tight to allow retraction. The ring contains elastic fibres that normally allow it to stretch over the glans.
Frenulum: A small band of tissue on the underside of the penis connecting the foreskin to the glans. The frenulum is rich in nerve endings and can sometimes be independently tight (frenulum breve), even when the rest of the foreskin functions normally.
Ridged band: A corrugated area near the foreskin tip containing Meissner's corpuscles (touch receptors). This is part of the tissue removed during circumcision.
Glans penis: The sensitive head of the penis, which is protected and kept moist by the foreskin. After circumcision, the glans remains exposed and gradually undergoes keratinisation (thickening of the outer layer), which affects its sensitivity profile—a key aspect of the adaptation process discussed later in this guide.
Blood Supply and Innervation
The foreskin has a rich blood supply from branches of the external pudendal arteries and is innervated by the dorsal nerve of the penis. During circumcision, careful attention is paid to achieving haemostasis (stopping bleeding), particularly around the frenular artery on the undersurface.
Phimosis
"Phimosis" means the foreskin won't retract over the glans. In adults, the key question is whether it's congenital (lifelong) or acquired — developed later due to scarring or inflammation.
That distinction affects both treatment and recovery — particularly sensitivity changes if your glans has been covered for decades.
Expand for the full congenital vs acquired breakdown and the implications.
Understanding Phimosis: Congenital vs Acquired
Phimosis—the inability to retract the foreskin over the glans—is one of the most common reasons for adult circumcision. However, not all phimosis is the same. Understanding whether your phimosis is congenital or acquired is important, as it influences both the approach to treatment and what you can expect from recovery.
Present from birth
In children, a non-retractile foreskin is normal—the foreskin and glans are fused at birth and naturally separate over time. By puberty, most boys can fully retract their foreskin.
However, in some individuals, this natural separation never fully occurs, or the preputial ring remains too narrow. These men reach adulthood having never been able to fully retract their foreskin.
Key features:
- Lifelong inability to retract
- Often assumed to be "normal"
- No history of infections or trauma as a cause
- May have adapted to the condition
Men with congenital (lifelong) phimosis present a unique clinical picture that deserves special attention. These individuals have never experienced normal foreskin retraction. Their glans has been continuously protected and unexposed throughout their entire life.
This has several important implications:
- The glans will be extremely sensitive.
- Having been protected from direct contact with clothing and the external environment for decades, the glans in these men is often exquisitely sensitive. This becomes highly relevant after circumcision.
- Sexual function has developed around the phimosis.
- These men have learned to experience sexual pleasure with their condition. While circumcision generally improves sexual function by removing the physical barrier, the transition involves a significant sensory adjustment.
- Hygiene challenges may have been lifelong.
- Complete cleaning beneath a tight foreskin is difficult or impossible. Some men with congenital phimosis have experienced recurrent smegma accumulation or low-grade inflammation without realising this is abnormal.
Develops later in life
Acquired phimosis occurs when a previously retractable foreskin becomes tight due to scarring, infection, inflammation, or skin disease. The foreskin may gradually become less mobile until retraction is no longer possible.
This is always considered pathological and typically requires intervention, as the underlying cause may be progressive.
Key features:
- Previously normal foreskin function
- Often associated with visible scarring
- May follow infections or trauma
- BXO is a common cause
Anatomy of the Foreskin (Prepuce)
The foreskin is a complex structure with several distinct anatomical components:
Outer foreskin: This is continuous with the skin of the penile shaft. It has a similar structure to normal skin, with keratinised epithelium that provides protection.
Inner foreskin: The mucosal surface that lies in contact with the glans. This tissue is thinner, more delicate, and contains a higher density of nerve endings than the outer surface. It produces secretions that help maintain moisture and reduce friction.
Preputial ring: The narrowest part of the foreskin opening. In phimosis, it is this ring that is too tight to allow retraction. The ring contains elastic fibres that normally allow it to stretch over the glans.
Frenulum: A small band of tissue on the underside of the penis connecting the foreskin to the glans. The frenulum is rich in nerve endings and can sometimes be independently tight (frenulum breve), even when the rest of the foreskin functions normally.
Ridged band: A corrugated area near the foreskin tip containing Meissner's corpuscles (touch receptors). This is part of the tissue removed during circumcision.
Glans penis: The sensitive head of the penis, which is protected and kept moist by the foreskin. After circumcision, the glans remains exposed and gradually undergoes keratinisation (thickening of the outer layer), which affects its sensitivity profile—a key aspect of the adaptation process discussed later in this guide.
Blood Supply and Innervation
The foreskin has a rich blood supply from branches of the external pudendal arteries and is innervated by the dorsal nerve of the penis. During circumcision, careful attention is paid to achieving haemostasis (stopping bleeding), particularly around the frenular artery on the undersurface.
Phimosis severity is commonly graded using the Kikiros classification, which helps guide treatment decisions and set realistic expectations:
- Grade 0: Full retraction with no tightness—this is normal
- Grade 1: Full retraction possible but tight behind the glans—may benefit from conservative treatment
- Grade 2: Partial exposure of glans possible—conservative treatment may be attempted but surgical options often needed
- Grade 3: Partial retraction with urethral meatus (opening) visible—usually requires surgical intervention
- Grade 4: Minimal retraction, meatus just visible—surgical intervention typically necessary
- Grade 5: Absolutely no retraction possible—circumcision is usually the most appropriate treatment
Men with Grade 4-5 phimosis (particularly when congenital) often have a more pronounced post-operative adaptation period, as the glans has had minimal or no exposure to external stimuli throughout life.
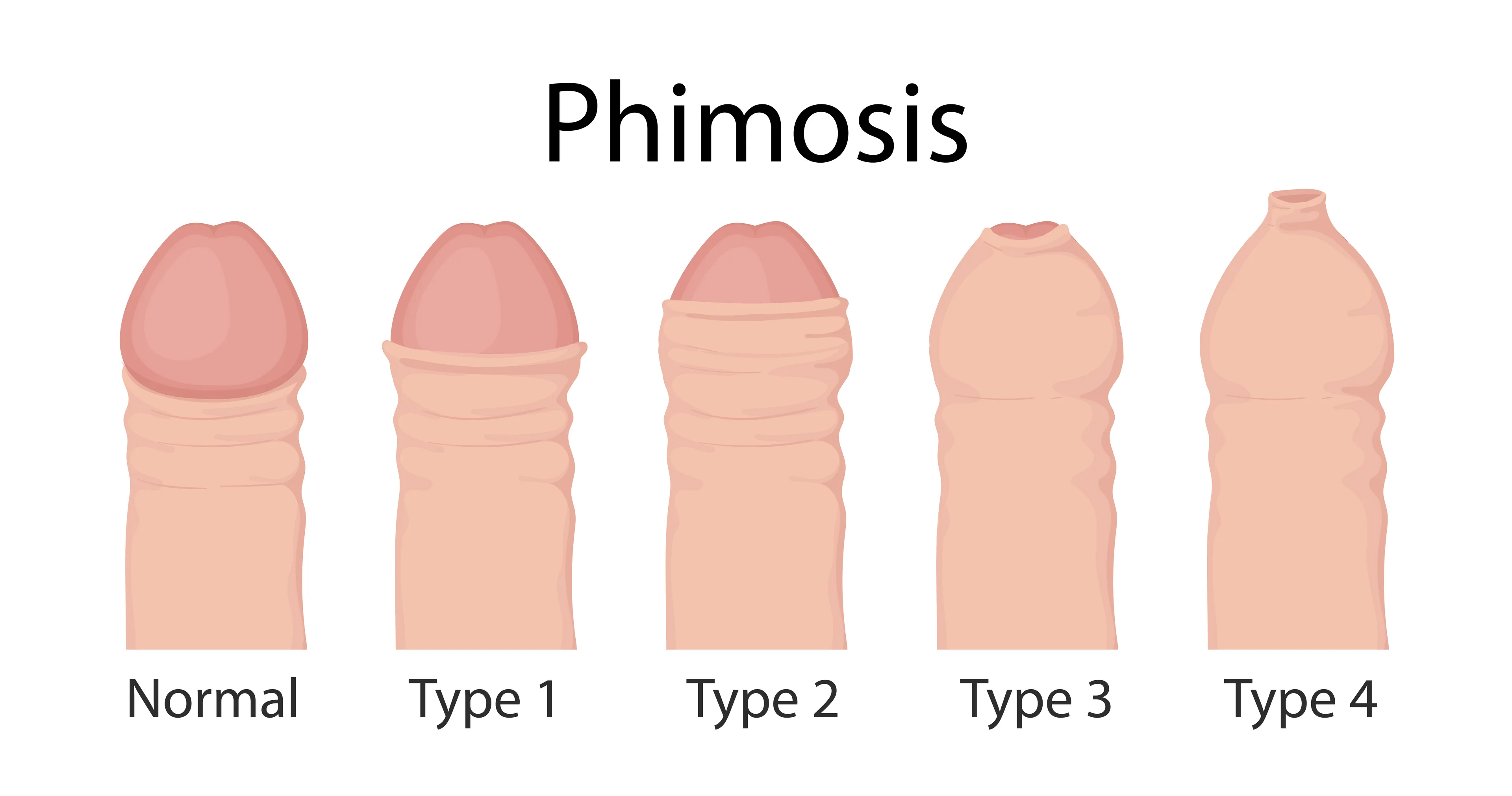
Visual Signs of Pathological vs Physiological Phimosis
In acquired (pathological) phimosis, the foreskin tip often appears:
- Whitish or pale (especially with BXO)
- Scarred or thickened
- Cracked or fissured
- Inelastic—doesn't stretch even with gentle pressure
In congenital phimosis without secondary pathology, the foreskin appears normal in colour and texture but simply has a narrow opening that has never widened.
Symptoms
Symptoms can be physical — tightness, pain, infections, urinary problems — or psychological, including distress, embarrassment, and avoidance of intimacy.
Expand for the full list and the “when it’s more than minor” context.
Symptoms of Phimosis
The symptoms of phimosis can range from mild inconvenience to significant distress. Common symptoms include:
- Difficulty or inability to retract the foreskin when the penis is flaccid or erect
- Pain during erections or sexual activity
- Tearing or bleeding of the foreskin during intercourse
- Recurrent episodes of balanitis (inflammation of the glans)
- Recurrent episodes of balanoposthitis (inflammation of the glans and foreskin)
- Unpleasant odour or discharge under the foreskin
- Ballooning of the foreskin during urination
- Urinary spraying or difficulty controlling the stream
- Inability to clean properly under the foreskin
- Psychological distress, embarrassment, or avoidance of intimacy
The presence of pain, infections, or difficulty urinating suggests that the phimosis is more than a minor issue. In these cases, a medical assessment is advised.
Phimosis severity is commonly graded using the Kikiros classification, which helps guide treatment decisions and set realistic expectations:
- Grade 0: Full retraction with no tightness—this is normal
- Grade 1: Full retraction possible but tight behind the glans—may benefit from conservative treatment
- Grade 2: Partial exposure of glans possible—conservative treatment may be attempted but surgical options often needed
- Grade 3: Partial retraction with urethral meatus (opening) visible—usually requires surgical intervention
- Grade 4: Minimal retraction, meatus just visible—surgical intervention typically necessary
- Grade 5: Absolutely no retraction possible—circumcision is usually the most appropriate treatment
When Phimosis Is More Than a Tight Foreskin
While phimosis itself is not dangerous, some underlying causes require careful evaluation. BXO in particular can occasionally be associated with precancerous changes, which is why the removed foreskin tissue is routinely sent for histological examination. If you notice any unusual changes in your foreskin—such as whitish patches, persistent sores, or areas that look different—it's important to seek assessment rather than delay.
Causes
Acquired phimosis develops through inflammation and scarring. Common causes include recurrent infections, skin conditions (especially BXO), diabetes, and trauma from forceful retraction.
Expand for the full list and why the underlying cause matters.
Causes of Acquired Phimosis
Acquired phimosis develops due to scarring or inflammation. Common causes include:
- Recurrent infections (balanitis or balanoposthitis), which cause inflammation and fibrosis over time
- Skin conditions such as BXO (also known as lichen sclerosus), which is a progressive inflammatory condition causing whitening, scarring, and narrowing of the foreskin
- Trauma from forceful retraction, sexual activity, or injury
- Diabetes, which increases the risk of recurrent infections and chronic inflammation of the foreskin
- Chronic irritation from poor hygiene, soaps, or persistent moisture
Identifying the underlying cause matters. For example, BXO may require specific management and histological confirmation, and it can affect other parts of the genital skin and urethra.
If you want to know more about BXO, click here:
Alternatives: The Conservative Management
Circumcision isn't the only option. The right approach depends on the type and severity of phimosis, your symptoms, and your priorities.
Expand for creams/stretching, preputioplasty, and frenuloplasty.
In selected cases—particularly mild to moderate congenital tightness—topical steroid creams combined with gentle stretching exercises can improve foreskin elasticity and allow retraction.
However:
- This approach is less effective in adults than in children
- It is usually not effective in acquired phimosis with scarring
- It is not appropriate if BXO is suspected
- Relapse is common if stretching is not maintained
Preputioplasty is a surgical procedure that widens the tight foreskin ring without removing the foreskin entirely. It can be an option for selected men who strongly wish to preserve their foreskin and have a suitable pattern of tightness.
Limitations include:
- Less definitive than circumcision
- May not be appropriate for severe scarring or BXO
- Risk of recurrence
- Cosmetic outcome is variable
In my practice, I discuss preputioplasty as an option when appropriate, but many men choose circumcision because it is the most definitive solution with the lowest risk of recurrence.
Important: Not All Treatments Are Suitable for Everyone
I will always be honest with you about which options are realistic for your specific situation. If you have BXO, significant scarring, or severe phimosis, I may recommend proceeding directly to circumcision rather than suggesting conservative treatments that are unlikely to succeed. This isn't about preferring surgery—it's about giving you realistic expectations and avoiding prolonged, ineffective treatment.
Circumcision: What happens during the surgery
You arrive. We confirm you're well, check consent, and mark the surgical plan agreed at consultation.
You lie on the operating table. I clean the area and inject local anaesthetic — the only painful part, lasting about 20 seconds. After that, you feel pressure and movement, but no pain.
I remove the foreskin using the agreed technique (sleeve resection in most cases), control any bleeding, and close with dissolvable stitches. The whole procedure takes 30–45 minutes.
You're awake throughout. We can talk, or not — your choice. Some men want distraction, some prefer quiet. There's no wrong answer.
If you'd rather be asleep, general anaesthetic is an option at certain locations. We'd discuss this at consultation.
After the procedure, I apply a dressing. You rest for 20–30 minutes, have a cup of tea, and go home. With local anaesthetic, you don't need anyone to collect you — though company is always welcome.
step-by-step and timing expectations.
Considering circumcision? Get a clear, specialist opinion.
A consultant-led assessment to confirm whether circumcision is appropriate for you, explain the surgical options, and discuss recovery honestly — without pressure to proceed.
CIRCUMCISION FAQ: The Procedure
The procedure itself: no. Local anaesthetic means you feel touch and pressure but not pain. The injection stings for about 20 seconds — that's the worst moment. Afterwards: yes, but it's manageable. Most men describe it as "uncomfortable" rather than "painful." Paracetamol and ibuprofen together work well. Days 3-5 tend to be the peak — swelling, sensitivity, the stitches feeling tight. Then it steadily improves. Night-time erections can be uncomfortable in the first two weeks. This is normal and not dangerous, though it might wake you up.
30-45 minutes for the procedure itself. Add 30 minutes before (preparation, anaesthetic) and 30 minutes after (rest, dressing check) — so allow about 2 hours total at the clinic.
I tailor the technique to your anatomy and preferences. The main variables are: How much inner foreskin to keep — more gives a "looser" result, less gives a "tighter" look Where the scar line sits — higher (more visible) or lower (hidden in the sulcus) Frenulum — keep it, reduce it, or remove it depending on your anatomy and whether it's causing problems We discuss all this at consultation. I'll ask what you want; you can ask what I recommend. It's your body — the decision is yours.
Here is what happens:, Preparation:, The area is cleaned and draped. Local anaesthetic is administered if you are having the procedure awake, or penile block is given after induction if under general anaesthesia. Assessment:, Any adhesions between the foreskin and glans are carefully separated if present (common in congenital phimosis)., Marking:, The circumcision line is planned carefully to ensure adequate tissue removal while preserving appropriate penile skin., Circumcision:, The foreskin is excised circumferentially at a level just behind the glans. Both the outer and inner layers are removed. Haemostasis:, Any bleeding vessels are carefully controlled using bipolar diathermy. The frenular artery is specifically addressed., Closure:, The skin edges are approximated and sutured with absorbable stitches that dissolve within 2–6 weeks. Dressing:, A light dressing may be applied, though this is not always necessary.
Recovery, Sensitivity and sexual function
Recovery is usually straightforward, but it takes time. Early swelling and bruising are common. Full healing typically takes 4–6 weeks.
Hypersensitivity of the glans is normal — especially if your foreskin was tight from birth and the glans has never been exposed.
Recovery timeline
Days 1-3: Swelling begins. Bruising is common. Keep the dressing dry. Rest.
Days 3-7: Swelling peaks. This looks alarming but is normal. The glans may look purple or dark — this is bruising, not circulation problems. Stitches feel tight.
Week 2: Swelling starts to reduce. Stitches begin dissolving (or fall out — both normal). You can shower normally now.
Weeks 3-4: Most swelling gone. Sensitivity settling. Looks closer to the final result, though not quite there yet.
Week 6+: Fully healed. Safe to resume all activities including sex.
The final cosmetic result takes 3-6 months as residual swelling resolves completely.
Expand for the full recovery expectations, hypersensitivity explanation, and practical tips.
Understanding what to expect after circumcision is crucial for a smooth recovery. I provide detailed written instructions to all my patients, but I want to be particularly thorough here because patient expectations significantly impact their experience.

Day 1–3: Immediate Post-operative Period
Some swelling and bruising is normal and expected. The glans will be very sensitive—this is particularly pronounced in men with lifelong phimosis. Any dressing should fall off naturally within 24 hours. Local anaesthetic from the penile block wears off within 6–12 hours, after which you may need simple painkillers.
Week 1: Early Healing
Swelling begins to reduce but remains noticeable. Sensitivity of the glans remains heightened—contact with clothing may feel intense or uncomfortable. Most men take 5–7 days off work. You can shower from day 2 but avoid soaking in baths. The suture line may look lumpy or irregular—this is normal.
Weeks 2–4: Tissue Healing
Stitches begin to dissolve and fall away. Swelling continues to improve. Glans sensitivity starts to moderate but remains higher than it will eventually be. You can resume light exercise. The exposed glans may appear dry or develop a thin scab—a thin layer of plain petroleum jelly can improve comfort and reduce friction.
Weeks 4–6: Wound Maturation
The wound should be fully closed. You can resume sexual activity once comfortable (typically from week 4–6). Some tightness during erections is normal initially and will ease. The scar begins to mature and soften. Sensitivity continues to gradually reduce.
Months 2–6: Neurological Adaptation
This phase is particularly important for men with lifelong phimosis. The glans continues to adapt to its new exposed state. Sensitivity progressively normalises as neurological pathways adjust. The keratinisation process (slight thickening of the glans surface) occurs naturally. Sexual sensation stabilises. Final cosmetic appearance achieved.
This Is Perhaps the Most Important Section for Men with Lifelong Phimosis
If you have had a tight foreskin your entire life, please read this section carefully. The post-operative adaptation period may be more challenging than you expect, but understanding what is happening—and why—makes it far more manageable.
Why Does Hypersensitivity Occur?
In men with lifelong (congenital) phimosis, the glans has been continuously protected by the foreskin since birth. It has never been directly exposed to clothing, air, water pressure in the shower, or the friction of daily movement. The surface of the glans in these men has a mucosal-type surface—thin, moist, and exquisitely sensitive.
After circumcision, this protected surface is suddenly exposed to constant stimulation. Every touch, every brush of clothing, every movement generates sensory signals that the nervous system has never had to process before. This is not damage—it is simply new input that the brain and peripheral nerves must learn to modulate.
What Does Hypersensitivity Feel Like?
Patients describe post-circumcision hypersensitivity in various ways:
- Intense awareness of the glans: A constant consciousness of the glans touching clothing, which can be distracting
- Discomfort with fabric contact: Some men find certain fabrics intolerable initially—the sensation may be described as burning, tingling, or overwhelming
- Shower sensitivity: Water pressure hitting the glans directly can feel surprisingly intense
- Sexual hypersensitivity: During masturbation or intercourse, sensation may be overwhelming rather than pleasurable initially
- Difficulty concentrating: The constant sensory input from the glans can be mentally exhausting in the early weeks
The severity varies considerably between individuals. Some men experience only mild, brief hypersensitivity. Others—particularly those with Grade 4-5 lifelong phimosis—may have significant symptoms lasting several months.
The Neurological Adaptation Process
What you are experiencing is your nervous system recalibrating. This is a well-understood neurophysiological process:
Peripheral adaptation: The nerve endings in the glans gradually reduce their responsiveness to constant stimulation through a process called sensory adaptation. Receptors that initially fire rapidly in response to touch progressively decrease their firing rate as the stimulus becomes familiar.
Central habituation: The brain learns to filter and deprioritise the constant sensory input from the glans. Initially, every signal gets attention. Over time, the brain recognises these signals as "background" rather than "alert" and stops bringing them to conscious awareness.
Keratinisation: The surface of the glans gradually thickens slightly as it adapts to exposure. This natural protective response provides a small physical barrier that reduces the intensity of stimulation reaching the nerve endings.
These three processes work together to progressively normalise sensation. It is important to understand that this is not "damage" or "loss"—your glans will still be sensitive and capable of sexual pleasure. What changes is the overwhelming nature of the sensation, which settles to a comfortable level.
Timeline for Neurological Adaptation
Based on my clinical experience with thousands of circumcisions:
- Weeks 1–2: Peak hypersensitivity. The glans is newly exposed and the nervous system has had no time to adapt. This is typically the most challenging period.
- Weeks 3–6: Gradual improvement. The initial overwhelming sensitivity begins to reduce. Most men notice significant improvement by week 4–6.
- Months 2–4: Substantial adaptation. For most men, hypersensitivity has largely resolved. Sexual function and comfort normalise.
- Months 4–6: Full adaptation for men with lifelong severe phimosis. Some patients require this longer period for complete neurological recalibration.
The key message: Even when symptoms are significant, they typically improve with time. In my experience, hypersensitivity settles for the vast majority of men. If it feels persistent, severe, or distressing, I'd rather you tell me early so we can support you.
While you cannot speed up neurological adaptation, you can make the process more comfortable:
- Vaseline/petroleum jelly: Apply a thin layer to the glans before dressing. This creates a protective barrier and reduces friction. Some men find this transformative.
- Soft, breathable underwear: Cotton is usually better tolerated than synthetic materials. Some men prefer snug briefs that hold the penis in a stable position; others prefer loose boxers that minimise contact.
- Non-adherent dressings: In the first 1–2 weeks, some men benefit from wearing a small non-adherent dressing (such as Mepitel or similar) over the glans, held in place by underwear.
- Gradual exposure: Counterintuitively, gentle, deliberate exposure (such as allowing water to run over the glans in the shower) can help accelerate adaptation compared to constantly protecting it.
- Patience: This may seem obvious, but understanding that the symptoms are temporary and typically resolve makes them far easier to tolerate psychologically.
Sexual Function During the Adaptation Period
Men are often understandably concerned about sexual function after circumcision, particularly given the hypersensitivity. Here is what to expect:
Initial period (weeks 1–6): Sexual activity should be avoided during wound healing. Once the wound is healed, you can resume sexual activity—but be aware that sensation will be different and potentially intense initially.
Early sexual experiences: Some men find that sexual sensation is overwhelming initially—stimulation that would previously have been pleasurable may be too intense. Others find the opposite—that the novel sensations are highly pleasurable. Many report finishing more quickly than before. This variability is normal.
Adaptation of sexual response: Over several months, sexual sensation normalises. The brain and peripheral nerves learn to process stimulation from the exposed glans appropriately. Most men report that their sexual function and satisfaction stabilises at a level equal to or better than before—but this takes time.
Lubrication, masturbation and partnered sex
After circumcision, the mechanics of sexual stimulation change. The foreskin normally provides a natural gliding movement over the glans; once it is removed, that movement is reduced.
For this reason, many men find that using an external lubricant during masturbation improves comfort and pleasure. Some also choose to use lubricant during partnered sex, particularly in the early months after surgery or when using condoms.
This is normal and does not indicate a problem or a complication. It reflects a period of adaptation to a different type of stimulation rather than a loss of sexual function. Over time, most men develop a new and entirely satisfying sexual routine.
Using lubricant is best understood as a practical adjustment, not a sign that something has gone wrong.
- Pain relief: Paracetamol and ibuprofen are usually sufficient. Take them regularly in the first few days rather than waiting for pain to become severe.
- Wound care: Keep the area clean. Shower from day 2, allowing water to run over the wound gently. Avoid soaking in baths or swimming for 3 weeks.
- Vaseline: Apply liberally to the glans to reduce sensitivity and prevent it sticking to underwear. This single measure makes the biggest difference to comfort for most men.
- Loose clothing: Wear comfortable, loose-fitting trousers when possible. Tight jeans can be uncomfortable in the first week or two.
- Erections: These are normal and will happen during recovery. They may feel tight or uncomfortable initially but will not damage the repair. Some men find that gentle pressure or thinking of something mundane helps if erections are troublesome at night.
- Work: Most men take 5–7 days off. Desk-based work can often resume within a week. Physically demanding jobs may require 2 weeks.
- Driving: Avoid driving for at least 48 hours after general anaesthetic. You can drive when you can comfortably perform an emergency stop.
- Sexual activity: Wait at least 4 weeks, or until the wound is completely healed. Using lubricant is recommended.
Circumcision permanently changes the appearance and, to some extent, the function of your penis. It's important to have realistic expectations about these changes.
Appearance
The most obvious change is visual—your glans will be permanently exposed. For men who have lived with phimosis, this may be the first time they have ever seen their own glans clearly. The circumcision scar is visible as a subtle line around the shaft behind the glans. The appearance continues to settle over several months as swelling resolves and the scar matures.
Sensation
As discussed extensively above, the glans will initially be hypersensitive before gradually adapting. Long-term, most men notice some change in sensation compared to their pre-circumcision state—but for men with severe phimosis who could not retract their foreskin, the comparison is not straightforward. Many report that their ability to enjoy sexual sensation is improved once they adapt.
Sexual Function
Based on current evidence, circumcision:
- Does not impair your ability to achieve erections
- Does not affect ejaculation mechanics or control
- Has no impact on fertility or sperm production
- Does not prevent satisfying sexual experiences (most men report long-term satisfaction)
What changes is the mechanics—the foreskin's gliding motion is absent, and the glans is directly stimulated. This is why many circumcised men find lubrication helpful. Sensation will be different, and it can take time to adapt—but different does not mean worse.
Hygiene
Many men find hygiene simpler after circumcision. There is no longer a foreskin to retract and clean beneath. For men who experienced recurrent infections due to difficulty maintaining hygiene, this can be transformative.
What about “loss of sensation”?
This is the question everyone wants answered but nobody wants to ask out loud.
The honest answer: Sensation changes — but "loss" is usually the wrong word.
The foreskin contains nerve endings. Removing it removes those nerve endings — that's factually true.
The glans — which has the highest concentration of sexual nerve endings — remains intact. Once exposed, it adapts over weeks to months through keratinisation, becoming less sensitive to friction.
What does this mean in practice?
- Most men report no meaningful difference in sexual pleasure
- Some report improvement, especially if phimosis was making sex difficult or painful
- A small number report reduced sensitivity that bothers them
- Some men with premature ejaculation find circumcision helps (though this isn't guaranteed and shouldn't be the main reason for surgery)
Individual variation is significant. I can't promise sensation will feel identical — but the overwhelming majority of men I've circumcised are satisfied with the outcome.
Sex and recovery after circumcision
What most men actually want to know
- Erections (including night-time erections) are expected and not harmful
- Swelling and sensitivity improve gradually over the following weeks
- Most men return to normal daily activities within a few days
- Sexual activity usually resumes once healing is complete (typically several weeks)
- Scarring usually softens and becomes less noticeable over time
We discuss realistic timelines, concerns, and individual variation openly before surgery.
CIRCUMCISION FAQs: Recovery
Desk job: 2-3 days. You'll be uncomfortable sitting for long periods initially, but it's manageable. Physical work (lifting, moving, sweating): 1-2 weeks minimum. Friction and sweat delay healing. Driving: when you can do an emergency stop without wincing. Usually 5-7 days. I'll give you a sick note if you need one.
6 weeks minimum. I know that's longer than you wanted to hear. The healing tissue is fragile. Friction causes micro-tears, bleeding, infection risk, and can affect the cosmetic result. Masturbation carries the same risks — wait the full 6 weeks. Some men heal faster and feel ready earlier. My advice: don't. The risks aren't worth the two-week head start.
Risks
Circumcision is generally safe when performed by an experienced surgeon. It is still an operation, so bleeding, infection, swelling, and delayed healing can occur.
Expand for the full list and context.
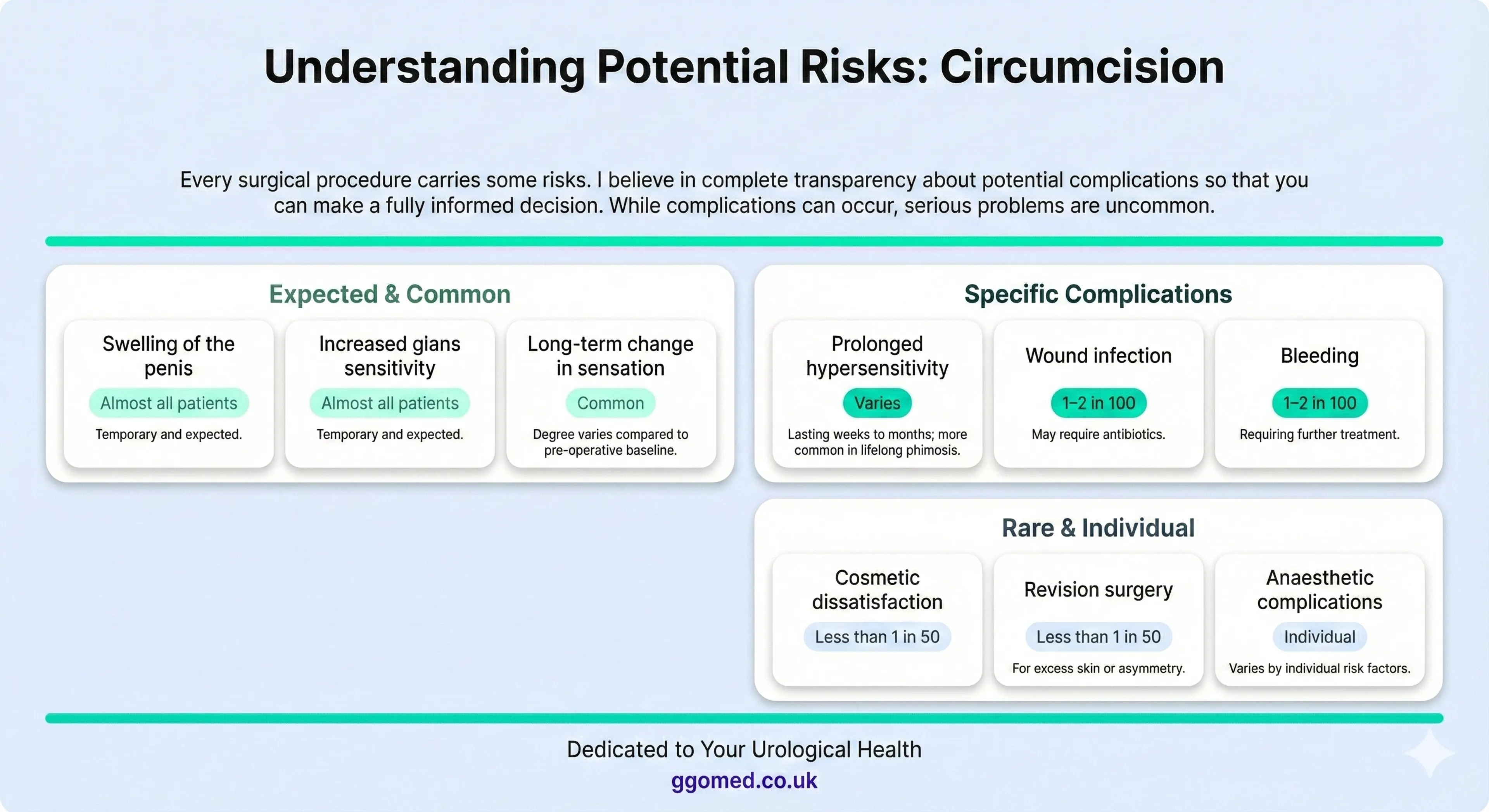
Risks and Complications
Adult circumcision is generally safe when performed by an experienced surgeon, but like any operation, it carries risks.
- Bleeding
- Infection
- Swelling
- Delayed wound healing
- Scar formation
- Cosmetic dissatisfaction
- Changes in sensation (usually temporary hypersensitivity, occasionally reduced sensitivity)
- Meatal irritation in the early weeks
Serious complications are uncommon. In my consultations, I explain risks clearly and in context, so you can make an informed decision.
Sensory Changes
The foreskin contains nerve endings that contribute to sexual sensation. After circumcision, some permanent change in sensation is expected. The nature of this change is highly individual—some men report reduced sensitivity (particularly to fine touch), while others report that sexual pleasure is enhanced once the initial hypersensitivity settles. Long-term studies show that most men remain satisfied with their sexual function after circumcision.
Bleeding
Some oozing in the first 24–48 hours is normal. Significant bleeding that soaks through dressings, or continued bleeding beyond the first day, may require review. In rare cases (approximately 1–2%), bleeding requires additional treatment—either pressure, re-suturing, or cauterisation. The risk is higher in men taking blood-thinning medications.
Infection
The genital area has a good blood supply and heals well, so infection rates are low. Signs of infection include increasing redness spreading from the wound, increasing swelling after the first few days, discharge of pus, fever, or feeling unwell. Prompt treatment with antibiotics is usually effective. Rarely, more extensive infection requires drainage or hospital admission.
Cosmetic Concerns
I aim for an aesthetically pleasing result, but minor asymmetry, slight irregularities in the scar line, or small skin tags can occur. The appearance continues to improve for several months as the scar matures. Rarely, excess skin (skin bridge) or significant asymmetry may require minor revision surgery.
Rare Complications (less than 1 in 250)
- Significant haematoma (blood collection) requiring drainage
- Wound breakdown requiring additional treatment
- Meatal stenosis (narrowing of the urinary opening)—more common after circumcision for BXO
- Buried penis (in patients with significant pubic fat pad)
- Injury to the glans (extremely rare)
- Persistent pain or discomfort
I discuss risks specific to your individual situation during the consultation, including how your anatomy, health conditions, and the underlying pathology may affect your risk profile.
When to Seek Medical Advice
While most recoveries are straightforward, contact us or seek medical attention if you experience:
- Increasing pain that is not controlled by regular paracetamol and ibuprofen
- Signs of infection: spreading redness, increasing swelling after the first few days, pus discharge, fever, or feeling unwell
- Significant bleeding that soaks through dressings or doesn't stop with 10 minutes of gentle pressure
- Difficulty passing urine or complete inability to urinate
- Wound separation or stitches coming apart with gaping of the wound edges
- Any concerns about your recovery that are worrying you
All my patients receive direct contact details for post-operative queries. If something doesn't feel right, get in touch. Early advice is always better than silent worry.
Next steps
If you're considering circumcision — whether you've had a tight foreskin for months or your entire life — a consultation is the best next step. We will:
- Examine you to confirm the diagnosis and assess the type and severity of phimosis
- Determine whether you have congenital or acquired phimosis, as this affects expectations
- Discuss whether circumcision is the right option for you, or whether alternatives may be appropriate
- Answer all your questions in a confidential, unhurried setting
- Explain exactly what to expect before, during, and after the procedure—including the adaptation period
- Provide a clear treatment plan and cost estimate
This is a personal decision, and there is no pressure. My role is to give you the information you need to make the right choice. If you've been living with this for years, it's not too late. Many patients tell me their only regret is not coming sooner.
How much does this actually cost?
Real prices. Real outcomes. No surprises.
Ready to Discuss about Your Circumcision?
Private, Confidential and Inclusive Consultation.
Further Resources
Useful External Links
Related Pages on This Site
References
- British Association of Urological Surgeons. "Circumcision (Complete Removal of the Foreskin)." Patient Information Leaflet A24/077. June 2024.
- Morris BJ, et al. "A 'snip' in time: what is the best age to circumcise?" BMC Pediatr. 2012;12:20.
- Krieger JN, et al. "Adult male circumcision: effects on sexual function and sexual satisfaction in Kisumu, Kenya." J Sex Med. 2008;5(11):2610-2622.
- Kigozi G, et al. "Foreskin surface area and HIV acquisition in Rakai, Uganda (size matters)." AIDS. 2009;23(16):2209-2213.
- Hayashi Y, et al. "Phimosis, paraphimosis, and circumcision." ScientificWorldJournal. 2011;11:289-301.
- Shabanzadeh DM, et al. "Male circumcision does not result in inferior perceived male sexual function – a systematic review." Dan Med J. 2016;63(7):A5245.
- Tian Y, et al. "Effects of circumcision on male sexual functions: a systematic review and meta-analysis." Asian J Androl. 2013;15(5):662-666.
- Celis S, et al. "Balanitis xerotica obliterans in children and adolescents: a literature review and clinical series." J Pediatr Urol. 2014;10(1):34-39.
- McGregor TB, et al. "Pathologic and physiologic phimosis: approach to the phimotic foreskin." Can Fam Physician. 2007;53(3):445-448.
- Yang SS, et al. "Highly potent and moderately potent topical steroids are effective in treating phimosis: a prospective randomized study." J Urol. 2005;173(4):1361-1363.
- Moreno G, et al. "Topical corticosteroids for treating phimosis in boys." Cochrane Database Syst Rev. 2014;9:CD008973.
- Cold CJ, Taylor JR. "The prepuce." BJU Int. 1999;83 Suppl 1:34-44.
- Sorrells ML, et al. "Fine-touch pressure thresholds in the adult penis." BJU Int. 2007;99(4):864-869.
- Bronselaer GA, et al. "Male circumcision decreases penile sensitivity as measured in a large cohort." BJU Int. 2013;111(5):820-827.
- Bossio JA, et al. "A review of the current state of the male circumcision literature." J Sex Med. 2014;11(12):2847-2864.
- Nordstrom MP, Wester T. "Timely intervention in boys with phimosis." Lancet. 2008;371(9626):1730-1731.
- Daling JR, et al. "Penile cancer: importance of circumcision, human papillomavirus and smoking in in situ and invasive disease." Int J Cancer. 2005;116(4):606-616.
- Van Howe RS, Cold CJ. "Human papillomavirus, circumcision, and penile cancer: an evidence-based assessment." Int J STD AIDS. 2013;24(5):362-370.
- Weiss HA, et al. "Male circumcision and risk of HIV infection in women: a systematic review and meta-analysis." Lancet Infect Dis. 2009;9(11):669-677.
Give your feedback and comment
Your circumcision will be performed personally by Mr Ollandini — not delegated.
