


I am a urological surgeon specialising in men's reproductive health. I regularly see people who are worried about how their varicocele — a swelling of the veins inside the scrotum — affects their active lifestyle. Perhaps you have noticed a dull ache after lifting weights, or wondered whether running is making things worse. Maybe you have questions about fertility. These are all reasonable concerns. Knowing how varicocele and exercise are linked can help you make better decisions. This guide explains what the evidence says.
This guide is designed for active people — whether you compete in sport, go to the gym regularly, run at weekends, or simply value staying fit. It builds on the main varicocele information with a focused look at sport-specific considerations, backed by the latest clinical evidence.
Get a personalised plan, not just information
Train with confidence — and protect fertility if it matters to you.
Train Smarter
what typically triggers ache:
Heavy lifting while holding your breath — this raises pressure inside your abdomen and can worsen symptoms
Long cycling sessions (saddle pressure + heat)
High-impact volume (lots of pounding + fatigue)
Know When to Test
when ultrasound / semen analysis adds value
You’re actively trying (or planning) for pregnancy
You have noticed that one testicle looks or feels different — smaller or softer than before
Symptoms are persistent or worsening despite support
A plan you can actually follow
Here is what we will decide together:
When monitoring is sensible
When training modifications are enough
When to discuss embolisation (a non-surgical method to block blood flow in the affected vein) vs surgery around your training cycle
What Happens During The Appointment
- Review symptoms (ache or heaviness, training triggers, fertility goals)
- Examination and grading (including a standing and Valsalva test — where you hold your breath and bear down gently — where appropriate)
- Decide what you actually need: scrotal ultrasound (a painless scan of the scrotum), semen analysis, or reassurance and monitoring
- Clear plan: training changes, symptom control, and if needed a discussion of embolisation (a non-surgical procedure to block the affected vein) vs microsurgical repair (a small operation to fix the veins using a microscope)
Recent Update: NICE and Varicocele for Fertility
NICE published its updated fertility guideline (NG257) on 31 March 2026, and it changed UK policy on varicocele treatment for people with fertility problems. Treatment — radiological or surgical — can now be considered where a varicocele is found on examination in someone trying to conceive with reduced semen parameters. For years the UK was the only country whose official guidance specifically advised against this, so the change matters.
Knowledge check
Quick check: Is it safe to train today?
Select the statement that best describes your situation right now.
Why Varicocele Makes Itself Felt During Sport
A varicocele (enlarged veins in the scrotum) often causes no symptoms at all — many people only notice it once they become more physically active. The link between exercise and varicocele symptoms is not a coincidence. It reflects how blood flows through the spermatic veins.
Is varicocele caused by sport?
The Valsalva Manoeuvre and Its Effects
When you lift something heavy, hold your breath during effort, or strain in almost any way, you naturally perform what's called a Valsalva manoeuvre. This involves closing the glottis (the space between your vocal cords) while attempting to exhale, which dramatically increases pressure in the chest and abdomen.
This pressure surge has several effects on the venous system. It temporarily impedes blood flow returning to the heart, causes engorgement of veins throughout the body, and specifically increases pressure in the testicular venous system. In someone with a varicocele—where the one-way valves in the testicular vein are already failing—this means more blood flows backward and pools in the dilated pampiniform plexus.
Why the Left Side Is Most Affected
You may have noticed that varicoceles almost always occur on the left side (approximately 85-90% of cases). This is due to anatomical factors: the left testicular vein enters the left renal vein at a perpendicular angle, creating greater resistance to flow compared to the right side, where drainage is more direct into the inferior vena cava. During exercise, this anatomical disadvantage becomes more pronounced.
Temperature Effects
Beyond pressure, physical activity also raises scrotal temperature—both through general body heat generation and through the mechanics of clothing and movement. Since the testes rely on being 2-4°C cooler than core body temperature for optimal function, and since varicoceles already impair the normal testicular cooling mechanism, exercise can compound the thermal stress on the testes. This has implications for both comfort and, potentially, for fertility in men who train intensively.
Does Exercise Make Varicocele Worse?
This is one of the most common questions I am asked in clinic, and I want to start with the honest answer: nobody has run the trial that would settle it. There is no study in which men with a varicocele were randomly assigned to train hard or train lightly and then followed up. So what follows is reasoning from how the veins behave, plus a small number of observational studies — not proof. For most people, regular moderate exercise is not thought to create a varicocele where none existed. Whether the type and intensity of training change the outcome for someone who already has one is genuinely uncertain, and it matters most to people who are also thinking about fertility.
What the guidelines actually say about exercise
Nothing. That is worth saying plainly. The two main sets of professional guidance — the European Association of Urology guidelines on sexual and reproductive health, updated in 2025, and the American Urological Association and American Society for Reproductive Medicine guideline on male infertility, updated in 2024 — cover how to examine, investigate and treat a varicocele. Neither tells men with a varicocele to stop lifting, stop running or stop cycling. There is no guideline recommendation to restrict exercise, because there is no evidence base that would justify one.
So when I suggest changing something about your training, I am treating your symptoms, not following a rule. If a change makes the ache better, it was worth making. If it does not, there is no reason to keep doing it.
One more point both guidelines do make, and it is relevant to active men who have had a scan: a varicocele that can only be seen on ultrasound and cannot be felt on examination — a subclinical varicocele — is not recommended for treatment. Neither guideline recommends scanning simply to look for one.
What science says about it
Common Myths About Exercise and Varicocele
Common Myths About Exercise and Varicocele ✗
Fact
Varicoceles develop due to inherent valve weakness in the testicular veins, often with a genetic component.
Heavy lifting doesn't create varicoceles, but it can make an existing one more noticeable by increasing venous pressure during exertion. Research shows that athletes without any baseline venous reflux develop new varicoceles at approximately the same rate as non-athletes. The apparent connection often arises because men become aware of symptoms during exercise—but the underlying condition was likely already present.
Fact
Reality Most men with varicocele can and should continue exercising. Moderate physical activity is beneficial for overall health and does not typically worsen outcomes. Some modifications may help manage symptoms.
The benefits of regular exercise for cardiovascular health, mental wellbeing, and metabolic function far outweigh the theoretical concerns about varicocele progression in most cases. The key is understanding which activities may require modification and listening to your body.
Fact
Pain is only one consideration. Varicoceles can affect testicular function and fertility even when painless. Men who are concerned about future fertility should consider assessment regardless of symptoms.
The impact on spermatogenesis (sperm production) can occur silently over time, particularly with intensive training that combines mechanical stress with increased scrotal temperature. A painless varicocele in an active man may still warrant monitoring, especially if fertility is a priority.
Fact
Both activities affect varicocele through different mechanisms, and which is "worse" depends on the individual. Running involves impact; cycling involves heat and saddle pressure. Neither is universally more problematic.
The truth is more nuanced: running creates repetitive jarring and may cause mechanical discomfort, while cycling involves prolonged seated position, perineal pressure, and increased scrotal temperature. Different men find different activities more or less tolerable depending on their specific varicocele characteristics.
Key Studies on Exercise and Varicocele Progression
Several studies have examined the relationship between physical activity and varicocele, providing useful clinical guidance:
The Zampieri Longitudinal Study (2011): This three-year study of adolescent boys found that regular sports participation (≥3 times/week) was associated with a significantly higher rate of subclinical varicocele progressing to clinical varicocele (36% vs 5%). However, sports did not increase the development of entirely new varicoceles in boys without baseline reflux.
The Rigano Study: Found that overall varicocele prevalence was not higher in athletes than non-athletes, but athletes with longer weekly training durations (7-12 hours/week) showed higher prevalence and severity than those training less—suggesting a dose-dependent relationship with training volume.
The Aldhafery Survey (2019): Examining 382 athletes in Saudi Arabia, found varicocele prevalence of 46% among screened individuals—higher than the general population rate of approximately 15%. Interestingly, all men with grade 3 varicoceles were training 5 days per week.
Clinical Interpretation
The evidence suggests that while moderate exercise doesn't cause varicoceles, very high training volumes and intensities may accelerate the progression of existing subclinical varicoceles. This has practical implications: if you're training at high intensity and have a known or suspected varicocele, closer monitoring may be warranted. If fertility is a current priority, adjusting training load during the conception period may be beneficial.
Get a Personalised Assessment
Every athlete's situation is different. A specialist consultation includes clinical examination, ultrasound review, and tailored advice for your training goals.
Gym and Weightlifting
Weight training is the activity most often linked to varicocele symptoms. When you lift heavy weights, pressure inside your belly rises sharply. This directly affects how blood drains away from the testicles.
Varicocele and Gym: a combo everyone talks about
Why Heavy Lifting Affects Varicocele
During heavy lifts, most people instinctively hold their breath and brace their core—the Valsalva manoeuvre. This is actually important for spinal stability and force production, but it creates enormous pressure in the abdominal cavity. Studies have measured intra-abdominal pressures during heavy squats and deadlifts reaching 150-200 mmHg or more—several times higher than resting levels.
This pressure wave reverberates through the venous system. In someone with competent venous valves, this is largely managed. In someone with varicocele, where valves are already failing, this pressure is transmitted directly to the testicular veins, causing further distension and blood pooling.
Exercises Most Likely to Trigger Symptoms
- Deadlifts — Particularly conventional deadlifts with heavy loads. The starting position and the requirement for sustained bracing make this particularly challenging.
- Squats — Both back and front squats, especially when working at high percentages of your maximum. The depth and load combine to create significant pressure.
- Overhead pressing — Standing presses require substantial core bracing, particularly at heavier weights.
- Heavy rows — Bent-over rows and other pulling movements from a hinged position.
- Leg press — Despite being a machine movement, the angle and loading can create substantial abdominal pressure.
Practical Modifications
Consider these evidence-informed strategies if weight training triggers your symptoms:
- Breathing technique: Rather than holding your breath throughout the entire rep, practice exhaling through the sticking point of the lift. This requires practice but can significantly reduce peak pressures while maintaining adequate core stability.
- Rep range adjustment: Working in moderate rep ranges (8-12 reps) at correspondingly lower weights typically generates less peak pressure than very heavy singles or triples, while still providing effective training stimulus.
- Exercise selection: Machine-based alternatives often allow similar muscle targeting with less requirement for extreme bracing. For example, leg extensions and hamstring curls instead of heavy leg press, or chest-supported rows instead of bent-over rows.
- Rest intervals: Longer rest between sets allows symptoms to settle before the next effort. If you're used to 60-90 second rests, try extending to 2-3 minutes on your heavier compound movements.
- Scrotal support: Wearing compression shorts or supportive underwear during training can reduce the mechanical pulling sensation many men experience.
A Note on Bodybuilding and Varicocele Prevalence
Some older literature has reported very high varicocele rates (60-80%) among competitive bodybuilders. While these figures may reflect selection bias in small samples, they highlight that chronic heavy training with sustained Valsalva effort does appear to be associated with higher varicocele prevalence and severity. If you're training at competitive bodybuilding levels and have fertility concerns, earlier intervention on your varicocele may be worth considering.
Running and Endurance Sports
Running affects a varicocele differently from weight training. Instead of sudden pressure spikes, endurance activities create steady, repeated stresses that build up over time. They also raise scrotal temperature during long efforts.
If you run and have a varicocele, you may notice symptoms are worse towards the end of longer runs, or in the hours after your session. Each footstrike sends a small jolt through the body. Over thousands of steps, this can cause discomfort. The friction and heat from movement also raises scrotal temperature — which matters for fertility.
The good news is that running does not usually cause the extreme pressure spikes that heavy lifting does. Many runners find they can keep training with small adjustments. But for those running at high volumes or with fertility concerns, understanding the build-up of effects over time is important.
The Impact Loading Effect
Each footstrike during running generates ground reaction forces typically equivalent to 2-3 times your body weight. This force is transmitted through your skeleton and soft tissues. For someone with a varicocele, this creates a repeated jarring effect on the testicular venous structures—each step is a small mechanical insult that, over the course of a 10km run (approximately 6,000-8,000 footstrikes), can accumulate.
This explains why many runners with varicocele notice symptoms more during the second half of longer runs: the cumulative effect of thousands of impacts eventually overwhelms the body's compensatory mechanisms.
Temperature Considerations
Running generates significant body heat, and the scrotal area is not exempt. Studies have shown that scrotal temperature rises during endurance exercise, and this rise is sustained for as long as activity continues. For runners training for an hour or more, this chronic heat exposure can be relevant:
- The testes require temperatures 2-4°C below core body temperature for optimal spermatogenesis
- Varicocele already impairs the normal counter-current cooling mechanism
- Prolonged running adds an additional thermal stress on top of this baseline impairment
This cumulative thermal effect has more relevance for fertility than for immediate symptoms, but it's worth understanding if you're a high-volume runner with fertility concerns.
Practical Approaches for Runners
- Supportive underwear: Compression shorts or running-specific supportive underwear can reduce mechanical oscillation and the "pulling" sensation many runners describe.
- Hydration: Good hydration helps maintain optimal blood viscosity and venous return. Dehydration thickens blood and may impede drainage.
- Terrain variety: Trail running or grass surfaces reduce impact compared to concrete, potentially lessening cumulative mechanical stress.
- Volume management: If symptoms are problematic, consider whether your training volume could be reduced without significant impact on your goals. Many runners find they can maintain fitness with slightly fewer weekly miles.
- Post-run recovery: Elevating legs after runs, cool showers, and allowing adequate recovery between sessions can help manage symptoms.
Marathon and Ultra-Endurance Considerations
For those training at very high volumes—marathon preparation or ultra-endurance events—the cumulative effects become more significant. Research on endurance athletes has shown transient drops in sperm count and motility after intensive training periods, with recovery typically occurring within days to weeks of reduced training. If you're preparing for a major event and also trying to conceive, timing your training cycles and conception attempts may be worth discussing with your specialist.
Cycling
Cycling creates a mix of problems for men with a varicocele. You sit for a long time. The saddle presses on the area between your legs (the perineum). And the temperature around your testicles rises and stays high. For these reasons, cycling deserves special thought — not to put you off riding, but to help you make smart choices about equipment and technique.
Unlike running or weight training, cycling affects a varicocele in several ways at once. The position squeezes blood vessels and nerves in the pelvic area. The saddle presses directly on the perineum. And the combination of padded shorts, body heat, and poor airflow means scrotal temperature can rise a lot during longer rides.
Saddle Pressure and Venous Congestion
The cycling position—particularly on road bikes with aggressive geometry—places significant weight on the perineum. This area contains blood vessels and nerves that can be compressed during riding. For someone with varicocele, this compression may impede venous drainage from the testicular region, potentially exacerbating venous pooling.
This explains why some cyclists notice varicocele symptoms are different from those experienced in other sports: less of the acute "pulling" sensation, more of a gradual congestion or heaviness that develops over the course of longer rides.
The Heat Factor
Cycling may be the sport with the greatest potential for sustained scrotal temperature elevation:
- Padded cycling shorts, while necessary for comfort, trap heat against the body
- The seated position keeps the scrotum close to the body and the saddle
- Unlike running, there's less natural ventilation from leg movement
- Longer rides (2+ hours) mean prolonged exposure
Research has documented significant scrotal temperature increases during cycling. For men with varicocele—where the normal testicular cooling mechanism is already impaired—this additional heat load can be particularly relevant for fertility considerations.
Practical Strategies for Cyclists
- Saddle selection: Consider saddles with cut-outs or channels designed to relieve perineal pressure. Many modern saddles are designed with this in mind, and finding the right one can significantly improve comfort.
- Bike fit: A professional bike fit can optimise your position to reduce pressure on sensitive areas. Even small adjustments to saddle height, angle, and position can make a meaningful difference.
- Standing intervals: Getting out of the saddle regularly during rides allows blood flow to return to normal and provides relief from sustained pressure.
- Shorts choice: While padding is necessary, some cycling shorts are better ventilated than others. Consider mesh panels or lighter-weight options for warmer conditions.
- Post-ride recovery: Allow time after rides before showering; a cool-down period helps scrotal temperature return to normal. Avoid immediately sitting in a car or continuing to compress the area.
A Positive Note: Horizontal Positioning
It's worth noting that cycling has one advantage over running: when you're on the bike, your body is more horizontal than when standing. This actually reduces the gravitational pooling effect on the varicocele. Some cyclists find that despite the heat and pressure issues, their varicocele is actually less symptomatic during riding than during running. Individual responses vary considerably.
Indoor cycling (turbo trainers, spin bikes) tends to create more scrotal heat than outdoor riding due to the absence of airflow. If you train extensively indoors and have fertility concerns, consider adding a fan directed at your lower body, taking regular breaks, and wearing lighter-weight shorts than you might outdoors.
Hyrox and Hybrid Fitness Competitions
Hybrid endurance and strength events like Hyrox combine continuous running with repeated high-effort tasks (sled push and pull, wall balls, farmers' carries, lunges). This creates a pattern that is very relevant for men with a varicocele.
- Sharp intra-abdominal pressure surges during strength stations — similar to the Valsalva-induced pressure patterns shown to aggravate venous reflux in the spermatic cord.
- Sustained running heat load, which increases scrotal temperature and can magnify the fertility impact of an existing varicocele.
- Repetitive impact and high weekly training volume, echoing athlete profiles in which varicocele progression and more pronounced seminal abnormalities have been documented.
Hyrox does not cause a varicocele in men with normal venous valves, but in those with known or subclinical varicocele, this type of training can:
- Unmask previously silent symptoms
- Worsen post-exercise aching or heaviness
- Accelerate progression from subclinical to clinical varicocele in high-volume athletes
- Compound fertility effects, especially in men training >5 days/week or combining endurance + heavy strength work
Practical recommendations for Hyrox athletes
- Use supportive compression shorts during training and racing to reduce venous pooling.
- Avoid prolonged maximal Valsalva during heavy stations; practise controlled exhalation under load.
- Consider modulating training blocks when trying to conceive, as both varicocele and intense endurance-strength training can impact sperm parameters.
- Seek assessment if training consistently triggers aching, heaviness, or marked asymmetry.
Hyrox is compatible with a healthy lifestyle, but men with known varicocele — or fertility plans — benefit from tailored management and periodic review.
Understanding Pain After Exercise
One of the most typical features of varicocele discomfort is its timing. Many men tell me they feel fine during their workout, but then notice symptoms building in the hours afterwards. Understanding why this happens can help you manage symptoms more effectively. It can also help you recognise what is normal versus what might need attention.
The delay happens because of how blood pools in the veins. During exercise, your muscles and raised heart rate keep blood moving. It is once you stop — when you are upright and still — that pooled blood in the dilated veins becomes most noticeable. Gravity now acts unopposed, and the blood that built up during exercise takes time to drain away.
Typical Symptom Progression
The classic pattern of varicocele symptoms after exercise follows a fairly predictable course:
- During exercise: May be asymptomatic, or may notice mild discomfort with specific movements (particularly heavy lifting or maximal efforts)
- Immediately after: Symptoms begin to emerge as you cool down and return to normal activities
- 1-3 hours post-exercise: Peak symptom intensity often occurs in this window—the characteristic dull ache, heaviness, or pulling sensation
- Evening: Symptoms typically persist or may worsen further if you've been on your feet
- Next morning: Symptoms usually resolve substantially after lying flat overnight
What Research Shows About Pain Intensity
A clinical study by Ebiloglu and colleagues quantified the relationship between exercise and varicocele pain. Among men with painful varicoceles, engaging in continuous physical activity caused mean pain scores to spike from approximately 3/10 at baseline to 7.5/10 post-exertion. This objective measurement confirms what many men experience subjectively—that exercise significantly amplifies varicocele discomfort.
Importantly, the same study showed that surgical treatment (varicocelectomy) was highly effective at resolving this exercise-induced pain, with microsurgical repair providing essentially complete relief in most cases.
Strategies for Managing Post-Exercise Symptoms
- Cool shower or bath: Cooling the scrotal area helps with vasoconstriction and symptom relief. Avoid hot showers immediately post-exercise.
- Elevation: Lying down with legs elevated for 10-15 minutes after exercise allows drainage and reduces symptoms.
- Supportive underwear: Continuing to wear supportive compression shorts in the hours after exercise can help.
- Gentle movement: Paradoxically, remaining completely sedentary can worsen symptoms. Light walking promotes venous return.
- Timing awareness: Plan activities requiring you to be on your feet for extended periods (standing events, long meetings) for days when you haven't trained heavily.
When to Stop Training and Seek Assessment
Seek Urgent Medical Attention
- Sudden, severe testicular pain (this could mean torsion — a medical emergency)
- Nausea or vomiting with testicular pain
- Testicle looks higher than usual or rotated
- Rapid swelling, especially if painful
- Pain with fever or urinary symptoms
Continue Training (With Awareness)
- A gradual, dull ache that gets better with rest
- Symptoms that follow the usual post-exercise pattern
- Discomfort that goes away overnight
- Heaviness without sharp or severe pain
- Symptoms that match what you have had before
- Zampieri N, Dall'Agnola A. Subclinical varicocele and sports: a longitudinal study. Urology. 2011;77(5):1199-1202.
- Di Luigi L, et al. Physical activity as a possible aggravating factor for athletes with varicocele: impact on the semen profile. Hum Reprod. 2001;16(6):1180-1184.
- Ebiloglu T, et al. The effect of physical activity on varicocele pain and resolution of this pain by different varicocelectomy techniques. Can J Urol. 2016;23(3):8285-8290.
- Aldhafery BF, et al. Prevalence and awareness of varicocele among athletes in Riyadh, Saudi Arabia. Res Rep Urol. 2019;11:231-238.
- Oranges F, et al. The Influence of an Intense Training Regime in Professional and Non-Professional Athletes on Semen Parameters: A Systematic Review. J Clin Med. 2025;14(1):201.
- Radojević N, et al. Restricting sports activity in reducing the rate of varicocele and related infertility parameters in athletes. Arch Med Sci. 2015;11(1):169-173.
- Practice Committee of the American Society for Reproductive Medicine. Report on varicocele and infertility: a committee opinion. Fertil Steril. 2020;114(6):1135-1142.
- National Institute for Health and Care Excellence. Fertility problems: assessment and treatment. NICE guideline NG257. Published 31 March 2026.
Fertility Considerations for Athletes
For men who are active and also worried about current or future fertility, the link between varicocele, exercise, and reproductive health deserves careful thought. The evidence suggests that intensive training may make the negative effects of varicocele on sperm worse — but also that these effects are often reversible with the right treatment.
Varicocele is the most common correctable cause of male infertility (difficulty having children). It affects around 40% of men who come forward with primary infertility. In athletes, the situation may be more complex. The combination of mechanical stress, heat, and oxidative stress (damage from intense training) can make the impact of varicocele on sperm production worse than either factor alone.
The "Double Hit" Effect
The idea comes from a study by Di Luigi and colleagues, published in 2001. They compared 120 men in four groups — athletes and non-athletes, with and without a varicocele — and found that the athletes with a varicocele had worse sperm movement and shape than the non-athletes with a varicocele. It is the study everyone cites, so it is worth knowing what it is and what it is not. It looked at each man at one point in time, it involved thirty men per group, and it is now over twenty years old. A study of that design can show that two things occur together; it cannot show that one caused the other, and it cannot tell you what would have happened to those same men had they trained less. My reading is that a compounded effect is plausible and unproven, and that is how I discuss it in clinic.
Heat, Oxidative Stress, and Sperm DNA Fragmentation
Three interconnected mechanisms explain how exercise and varicocele combine to affect fertility:
Thermal stress: Spermatogenesis is exquisitely sensitive to temperature. The testes evolved to sit outside the body cavity specifically because they require temperatures 2-4°C below core body temperature for optimal function. Varicocele impairs the normal counter-current cooling mechanism of the testicular blood supply. Intensive exercise—particularly endurance sports and cycling—adds an additional heat load. The combination can create sustained periods of elevated testicular temperature that impair sperm production and quality.
Oxidative stress: Intense exercise generates reactive oxygen species (ROS) throughout the body as a byproduct of high metabolic activity. While the body has antioxidant defences, these can be overwhelmed during very heavy training. Varicocele independently increases oxidative stress in the testicular environment through hypoxia and venous stasis. Athletes with varicocele may therefore experience a "double hit" of oxidative damage to their sperm.
Sperm DNA fragmentation: Both heat and oxidative stress can damage sperm DNA. High DNA fragmentation index (DFI) is associated with reduced natural conception rates and poorer IVF/ICSI outcomes. Research has shown that varicocele repair can reduce sperm DNA fragmentation, suggesting this mechanism is treatable.
What the Studies Show
The Di Luigi Study: This pivotal research compared four groups: athletes and non-athletes, with and without varicocele. Key findings:
- Athletes with varicocele had lower progressive sperm motility than non-athletes with varicocele
- Morphologically normal sperm percentage was approximately 34% in athletes with varicocele versus 42% in non-athletes with varicocele
- Only the athletic varicocele group showed significant testicular volume discrepancy (left hypotrophy)—a marker of varicocele-induced testicular damage
- Importantly, resting hormone levels were similar across groups, suggesting local testicular effects rather than systemic hormonal disturbance
The Radojević Study: Adolescent athletes with varicocele who stopped sports for six months showed:
- Significant improvements in sperm concentration and motility
- Complete resolution of varicocele in 18 out of 49 athletes
- One-grade improvement in varicocele in a further 19 athletes
This study provides particularly valuable evidence that training-related varicocele effects can be at least partially reversible.
Clinical Implications for Active Men
For athletes with varicocele who are concerned about fertility, several evidence-based strategies emerge:
- Earlier consideration of varicocele repair: Given the compounded effect of intense training on varicocele-related fertility impairment, proactive treatment may be particularly beneficial in very active men.
- Training load modification during conception attempts: Temporarily reducing training intensity and volume while trying to conceive may improve sperm parameters. This is a time-limited intervention that need not permanently affect your athletic goals.
- Heat management: Specific attention to scrotal cooling—avoiding hot baths, using cooling strategies during indoor training, choosing lighter shorts—may help protect sperm production.
- Antioxidant consideration: While the evidence for antioxidant supplements is mixed, some specialists recommend them for active men with varicocele and fertility concerns. Discuss this with your treating physician.
- Semen analysis monitoring: Regular semen analysis (every 6-12 months) allows tracking of any changes and informs decisions about timing of intervention.
The NICE Guidelines Shift
NICE published its updated fertility guideline (NG257) on 31 March 2026 — the first full revision of the UK guidance since 2013 — and it changes the position materially. NICE now advises considering radiological or surgical treatment of a varicocele that is detected on clinical examination in people trying to conceive spontaneously who have reduced semen parameters, with the decision taking female fertility factors into account as well. For years the UK stood alone in guidance that specifically discouraged this treatment, so this is a genuine shift rather than a restatement. For an athlete with a clinical varicocele and fertility concerns, it means treatment can now be discussed earlier and on firmer ground. What NG257 does not yet settle is timing — when in a couple's journey, and where in a training year, repair is best undertaken — so that part of the decision remains an individual one.
Palpable or subclinical: the distinction the guidelines insist on
This page spends a good deal of time on subclinical varicoceles — the small ones seen only on a scan — because they are what an active man is most likely to have quietly progressing. It is therefore important to be clear about what the guidelines do and do not support treating.
The American Urological Association and the American Society for Reproductive Medicine, in their joint guideline (2020, amended 2024), advise considering surgical varicocele repair in men trying to conceive who have a varicocele that can be felt on examination, together with infertility and abnormal semen parameters — a moderate recommendation resting on Grade B evidence. For a varicocele that is only visible on ultrasound and cannot be felt, the same guideline recommends against repair: the evidence does not show a benefit. The European Association of Urology, in its 2025 update on male infertility, takes the same view on subclinical disease.
In practice this means that a scan finding alone is not a reason to operate, however hard you train. What earns closer attention in an athlete is a varicocele that has become palpable, semen parameters that have fallen, a testicle that has lost volume, or pain that no longer settles. Those are the findings that turn a monitoring conversation into a treatment conversation.
Knowledge check
Which factor does NOT typically contribute to reduced fertility in athletes with varicocele?
Knowledge check
Research suggests that when athletes with varicocele stop intensive training for six months:
Fertility Concerns?
Semen analysis and fertility assessment available as part of your consultation. Let's discuss your options while you continue training.
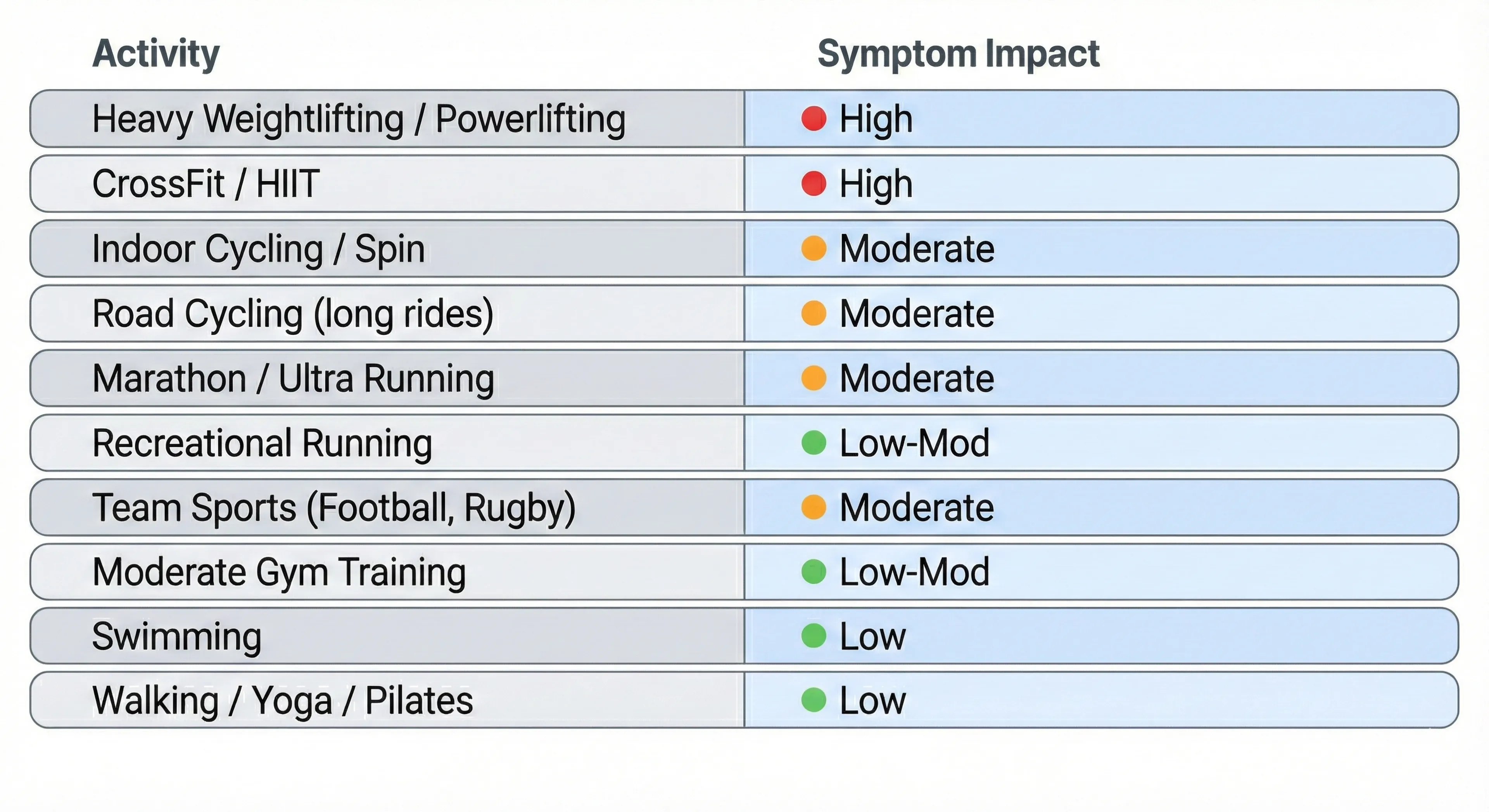
Sports Impact Index
Not all sports affect a varicocele in the same way. The guide below gives a general idea of how different activities tend to affect symptoms and fertility. Remember that everyone responds differently — some men cope well with activities others find difficult.
Did you know?
Interestingly, research suggests swimming may actually be protective against varicocele development and progression. A study comparing water-polo players to other athletes found that the aquatic group had a lower incidence of varicocele (approximately 9%) than even the non-athlete control group (approximately 12%).
Why Swimming May Be Beneficial
- Horizontal positioning: Swimming reduces gravitational pooling in the scrotal veins
- Water cooling: Immersion in water (especially cooler water) keeps scrotal temperature low
- No Valsalva strain: Swimming involves minimal breath-holding under strain compared to weight training
- Hydrostatic pressure: Water pressure may actually assist venous return
For men with varicocele who want to maintain high fitness levels while minimising symptom aggravation, swimming can be an excellent option. Many patients report that it's one of the few vigorous activities that doesn't worsen their symptoms—and some find it actually provides relief. This is a consistent clinical impression rather than a finding from a randomised trial, and the supporting water-polo observation is a single study awaiting replication.
When to Seek Specialist Assessment
While many men with varicocele successfully manage their symptoms alongside an active lifestyle, there are circumstances where specialist assessment becomes particularly valuable. As a urologist with a focus on andrology, I see patients across a spectrum—from those seeking reassurance that their approach is sound, to those requiring intervention to protect their fertility or quality of life.
Assessment is particularly worthwhile when symptoms begin to interfere with training enjoyment or consistency, when fertility is a current or future priority, or when you've noticed changes that concern you. A specialist consultation typically involves clinical examination, ultrasound imaging, and—where relevant—semen analysis, providing a complete picture of your individual situation.
When to Seek Specialist Assessment
Many men with a varicocele manage their symptoms well alongside an active lifestyle. But there are times when seeing a specialist is particularly worthwhile. As a urologist with a focus on andrology, I see patients across a wide range — from those who just want reassurance, to those who need treatment to protect their fertility or quality of life.
A specialist assessment is especially useful when symptoms start to affect your training, when fertility is a current or future priority, or when you have noticed changes that concern you. A consultation usually includes a physical examination, an ultrasound scan, and — where relevant — a semen analysis. Together, these give a full picture of your individual situation.
Not sure if your symptoms warrant assessment?
Many athletes I see weren't sure either. A consultation clarifies whether you need intervention or can continue training with modifications — and gives you a clear plan either way.
Return to Sport After Varicocele Treatment
For athletes who have varicocele repair — whether microsurgical varicocelectomy (surgery) or embolisation (a non-surgical procedure) — a key question is how quickly and safely they can return to training. Recovery is usually quick, and most men are back to full activity within about four to six weeks. I should be clear that this window comes from what surgeons see in practice and from custom, not from trials that tested one timetable against another. Nobody has shown that returning at four weeks is safer or worse than returning at six.
The recovery timeline depends on the procedure used and the intensity of sport you plan to return to. What follows is a general guide. Your surgeon's specific instructions should always come first, as they are tailored to your individual procedure and circumstances.

Plan your surgery around your competition calendar
Detailed Recovery Guidance
Microsurgical Varicocelectomy Recovery
Microsurgical inguinal or subinguinal varicocelectomy involves a small cut in the groin. The dilated veins are carefully tied off under magnification. Recovery is generally straightforward:
- Mild scrotal swelling and discomfort usually settles within days
- The wound heals over 10 to 14 days; stitches are usually dissolvable
- Most patients can return to desk work within a week
- Full recovery for sport is usually reached by 4 to 6 weeks
Embolisation Recovery
Varicocele embolisation is carried out by an interventional radiologist. They reach the testicular vein through a small puncture in the neck or groin. Recovery is often faster than surgery:
- No groin cut means less discomfort at first
- Many patients return to light activity within days
- Light exercise is often allowed within 1 to 2 weeks
- Full return to sport may be possible by 3 to 4 weeks
There is a trade-off between the two. Embolisation avoids a cut and has a good safety record, but the varicocele comes back more often afterwards — published series put recurrence at around 13 in 100, and in some cases the vein cannot be reached at all, so the procedure does not go ahead. Microsurgical repair has the lowest recurrence rate of the available techniques, which is why the European guidelines regard it as the most effective option. Neither is the right answer for everyone. Your surgeon can talk you through which fits your situation.
Sport-Specific Considerations
Weightlifting: The exercises most affected by varicocele — heavy compound lifts with breath-holding — should be the last to come back into your programme. Start with machines and lighter weights. Build up over 2 to 3 weeks once you are cleared for full training.
Running: You can usually start jogging again by weeks 3 to 4, and normal running by weeks 5 to 6. The impact may cause mild awareness of the surgical area at first. This usually settles quickly.
Cycling: Once wounds are fully healed (usually by week 3), you can start cycling again. Begin with shorter rides and make sure the saddle is comfortable before returning to longer distances.
Contact sports: Wait until 6 weeks, or until your surgeon says it is safe. Wearing a protective cup is a good idea for the first few months after you return.
What to Expect After Recovery
Many men find the exercise-related ache they had before surgery is much reduced or gone afterwards, but I cannot promise you that outcome. In a published series of 132 men who had microsurgical repair for testicular pain, 83 in every 100 had their pain resolve completely; the remaining 17 still had pain, and in that group it was still moderate. Pain on one side only did better than pain on both sides. So the odds are reasonably good, and a real minority are not helped. That is the conversation to have before you decide.
For fertility, improvements in sperm results usually become visible around 3 months after the operation. This reflects the full sperm production cycle. A follow-up semen analysis at 3 to 6 months allows you to see whether things have improved.
Practical Strategies for Training with Varicocele
Whether you are waiting for treatment, have chosen to manage things conservatively, or simply want to train as comfortably as possible, the following evidence-informed strategies can help you keep enjoying physical activity with a varicocele.
A note on what these strategies rest on
Take supportive underwear as the example. Snug support, a jockstrap or a firm-fitting brief is one of the first things men are told to try, and many say it helps. There is, as far as I can find, no proper trial of it in varicocele — no study comparing supportive underwear with ordinary underwear and measuring what happened. A great deal of what is written online about specific varicocele underwear, complete with percentages, is marketing rather than research. So: it is cheap, harmless, and worth trying for a few weeks. If it helps you, keep it. That is the whole basis for the advice, and I would rather you knew that than believed it was proven.
The same applies to the rest of it — cooling down after long rides, adjusting a saddle, breathing out through a heavy lift instead of holding your breath, easing back on volume for a few weeks to see what changes. These are sensible, low-cost experiments based on how the veins and the temperature around the testicles behave. They are not treatments with proven results, and none of them corrects the vein itself. Judge each one by whether it makes you feel better.
Key Principles
- Support: Reducing mechanical stress on the varicocele
- Technique: Minimising unnecessary pressure during exertion
- Cooling: Managing scrotal temperature, particularly for fertility
- Recovery: Optimising drainage after exercise
- Awareness: Recognising what's normal and what warrants attention
Supportive Underwear and Compression
Appropriate support can significantly reduce the mechanical "pulling" sensation many men experience during exercise:
- Compression shorts: Purpose-designed athletic compression shorts provide support without being restrictive. Look for quality materials with adequate elasticity.
- Jockstrap: Traditional athletic supporters remain an effective option, particularly for high-impact activities or when extra support is needed.
- Running shorts with liner: Built-in brief liners provide some support; consider layering with compression shorts for longer runs if symptoms are problematic.
- Avoid loose underwear during exercise: Standard boxers provide minimal support and allow the varicocele to move freely—not ideal during physical activity.
Breathing and Technique for Weight Training
- Practice controlled exhale: Rather than holding your breath throughout heavy lifts, practice exhaling through the sticking point. This takes practice but can meaningfully reduce peak intra-abdominal pressure.
- Avoid prolonged breath-holds: Multiple reps without breathing creates sustained pressure. Breathe between reps.
- Consider a belt strategically: Weight belts can actually increase intra-abdominal pressure (that's partly their purpose). Consider whether you truly need one, or whether it's exacerbating symptoms.
- Exercise selection: Where possible, substitute exercises that require less extreme bracing. Machines often allow similar targeting with reduced pressure demands.
Temperature Management (Particularly for Fertility)
- Avoid hot baths/saunas post-exercise: A cool or lukewarm shower is preferable. Hot immersion adds thermal stress when the testes are already warmed from exercise.
- Indoor training considerations: Add a fan directed at your lower body during indoor cycling or gym sessions. The absence of outdoor airflow means heat accumulates more rapidly.
- Clothing choice: Looser, lighter-weight shorts may be preferable to heavily padded or tight options, particularly in warm conditions. Balance support needs with ventilation.
- Post-exercise cooling: Allow time in a cool environment after training before showering or sitting. This helps scrotal temperature return to normal.
Post-Exercise Recovery Strategies
- Elevation: Lying down with legs elevated for 10-15 minutes after exercise promotes venous drainage and can reduce post-exercise symptoms.
- Cool shower: Cooling the scrotal area helps with vasoconstriction and symptom relief.
- Gentle movement: Complete immobility after exercise can actually worsen venous pooling. Light walking in the hours after training helps maintain circulation.
- Adequate rest days: If symptoms are significant, ensure you're allowing adequate recovery between sessions. Chronic accumulated stress may be worse than any single session.
Training Programme Adjustments
- Volume vs intensity: If symptoms are problematic, consider whether you can achieve your goals with slightly lower intensity and higher volume, reducing peak pressure demands.
- Exercise order: Front-loading your most challenging exercises when you're fresh, rather than leaving heavy compounds until you're fatigued, may reduce total stress.
- Activity variety: Incorporating lower-impact activities (swimming, cycling with good saddle setup) alongside higher-impact training can maintain fitness while providing symptom relief days.
- Fertility-focused timing: If actively trying to conceive, consider timing your highest-volume training blocks for periods when conception is not being attempted, and moderating training during fertility windows.
Athlete timeline: training and recovery
- If no procedure: you usually keep training with modifications and support garments
- If embolisation or surgery is considered: we discuss time off heavy lifting, return to running, and what to do during the fertility window
- If fertility is the priority: we align testing and timing (the trend in semen analysis matters more than panic)
This guide has been shaped by the concerns and experiences patients have shared with me in clinic over the years. The questions you ask—whether about training modifications, fertility implications, or recovery timelines—directly inform what I include and how I explain it. If you have questions this page hasn't answered, or if your experience with varicocele and sport offers insights that might help others, I'd genuinely value hearing from you.
Ask a Question
If something on this page is unclear, or if you have a question I haven't addressed, you're welcome to get in touch. While I can't provide individualised medical advice without a proper consultation—your specific situation requires proper assessment—questions that might help other readers may be incorporated into future updates to this page.
Common themes from patient questions have already shaped sections on post-exercise pain timing, the "myths versus facts" clarifications, and the sport-specific practical modifications. Your question might help the next person seeking the same information.
Share Your Experience
If you've navigated varicocele as an active person—whether managing symptoms conservatively, modifying your training approach, or returning to sport after treatment—your experience could help others feel less alone with this condition.
Many men tell me they felt isolated when first researching varicocele and sport, uncertain whether their symptoms were normal or whether their concerns were valid. Hearing from others who've been through similar experiences can be genuinely reassuring.
I'm considering adding an anonymous patient experiences section in future updates to this guide. If you'd be interested in contributing a brief account of your journey—what worked, what didn't, what you wish you'd known earlier—please let me know.
Was This Guide Helpful?
Feedback helps me understand what's working and what could be improved. If this guide has answered your questions, helped you make decisions about your training or treatment, or simply reassured you that your concerns are valid, I'd appreciate knowing.
Equally, if you found sections confusing, felt important topics were missing, or think the tone didn't quite land, constructive feedback helps me serve future readers better.
You can reach me through the contact form on this website, or mention this page when booking a consultation if you'd like to discuss your situation in more depth.
A Note on Online Discussions
I'm aware that varicocele is actively discussed on social media platforms and forums, with men sharing experiences, concerns, and sometimes conflicting advice. Some of these discussions raise valid questions; others promote treatments with limited evidence or generate unnecessary anxiety.
If you've come to this page after reading worrying posts elsewhere—perhaps about exercise "destroying" fertility or varicocele being a "silent threat"—I hope the evidence-based perspective here has been helpful. The reality is usually more nuanced than alarming headlines suggest, and most men with varicocele can continue enjoying active lifestyles with appropriate awareness and, where needed, effective treatment.
Practice Transparency: Fees and Prices
Radical transparency means that I will always be clear and upfront about the costs and the fees you are going to face.
LIMITATIONS AND UNCERTAINTIES
What We Do Not Yet Know: Limitations of the Evidence
As with all areas of medicine, our understanding of varicocele and sport is still developing. I believe in being open about what the research tells us with confidence, and where genuine uncertainty remains.
Here is the short version of what we do not know. No trial has tested whether changing your training changes anything about a varicocele — symptoms, sperm results or the vein itself. No trial has tested supportive underwear. No guideline recommends restricting exercise. The evidence that hard training worsens a varicocele's effect on sperm rests largely on one small study from 2001 that cannot establish cause. The return-to-sport timings after repair are surgical convention rather than tested schedules.
What we do know reasonably well is narrower: how a varicocele is diagnosed and graded, that treating a subclinical one is not recommended, that microsurgical repair has a lower recurrence rate than embolisation, and roughly how often surgery relieves pain. Where this page gives you advice beyond that, treat it as reasoning applied to your situation, to be tested against how you actually feel — not as fact.
Most studies examining varicocele and exercise are observational rather than randomised controlled trials. This means we can identify associations—for instance, that athletes with varicocele have worse semen parameters than non-athletes with varicocele—but we cannot definitively prove that exercise caused the difference. There may be confounding factors we haven't fully accounted for.
The Zampieri longitudinal study is one of the few that followed participants prospectively over time, providing stronger evidence for a causal relationship between sports participation and varicocele progression. However, it focused on adolescents rather than adult athletes, and we cannot assume findings translate directly across age groups.
Sample sizes in many studies are relatively small, and populations studied (often young men in specific countries or sports) may not fully represent the diversity of men seeking guidance.
The impact ratings I've presented synthesise evidence from multiple sources, including peer-reviewed studies, clinical experience, and patient reports. They are not derived from a single definitive study comparing all activities head-to-head under identical conditions—no such study exists.
Individual responses vary considerably. Some men tolerate activities I've rated as "high impact" with minimal symptoms, while others find "low impact" activities unexpectedly problematic. Your anatomy, varicocele grade, baseline fitness, training technique, and numerous other factors all influence your personal response.
The ratings should guide initial thinking and inform conversations with your clinician—they should not be interpreted as absolute restrictions. If an activity feels comfortable and isn't interfering with your goals, the classification on a general index matters less than your lived experience.
While we have reasonable evidence that varicocele affects semen parameters and that intense exercise can compound this effect, long-term conception outcomes in athletes with treated versus untreated varicoceles remain less well-studied than we'd like.
Most fertility research uses semen parameters—sperm count, motility, morphology, and sometimes DNA fragmentation—as surrogate endpoints rather than actual pregnancy rates. These parameters correlate with fertility but don't perfectly predict it. A man with moderately impaired parameters may conceive without difficulty; another with better numbers may struggle. The relationship is probabilistic rather than deterministic.
The optimal timing of varicocele treatment relative to training cycles, the magnitude of benefit from temporary training reduction during conception attempts, and the interaction between varicocele treatment and assisted reproduction outcomes all warrant further research.
Several questions remain genuinely unsettled in the literature:
Whether swimming is truly protective against varicocele or simply neutral compared to sedentary controls. The water-polo study is intriguing but represents a single observation that requires replication.
The exact threshold of training volume or intensity where risk becomes clinically significant. Current evidence suggests a dose-response relationship, but we cannot specify precise cut-offs with confidence.
Whether temporary training reduction during conception attempts independently improves outcomes, or whether its benefit is primarily mediated through allowing varicocele treatment and recovery.
The relative contribution of heat, oxidative stress, mechanical factors, and hormonal fluctuations to exercise-related fertility effects—and whether targeting specific mechanisms (for instance, with cooling strategies or antioxidants) can meaningfully mitigate risk.
These limitations don't mean the guidance on this page is unreliable. The core principles—that intense exercise can unmask or accelerate existing varicoceles, that symptoms characteristically worsen after activity, that fertility effects may compound in very active men, and that treatment is highly effective—are well-supported by consistent evidence across multiple studies.
However, the limitations underscore why individualised assessment matters. Your specific situation may differ from study populations in important ways. Decisions about monitoring, training modification, or treatment should be made collaboratively with a specialist who understands both the evidence and your personal circumstances, goals, and values.
If you're uncertain how to weigh the evidence in your situation, or if you'd like to discuss what these limitations mean for your specific case, I'm happy to explore them during a consultation.
FAQs
For most men, moderate exercise does not worsen varicocele in terms of progression or long-term outcomes. However, certain high-intensity activities—particularly heavy weightlifting with Valsalva—can make symptoms more noticeable and may accelerate the progression of existing subclinical varicoceles in some cases. The key distinction is between experiencing symptoms during/after exercise (which is common and manageable) versus actually worsening the underlying condition (which requires more intensive training over longer periods to occur). General fitness activities are not harmful and have many benefits that outweigh any theoretical varicocele concerns.
The decision about varicocele surgery depends on your symptoms, fertility concerns, and personal circumstances—not specifically on whether you're an athlete. However, if symptoms are significantly interfering with training, or if you're concerned about fertility while continuing high-intensity exercise, treatment may be particularly beneficial. The recovery period (4-6 weeks) is relatively short, and most athletes report improved comfort and ability to train after successful repair. This is a decision best made with specialist advice tailored to your situation.
Most men can return to light gym activity by 2-3 weeks post-operatively, with progression to full training by 4-6 weeks. Heavy compound lifts (deadlifts, squats) should be the last exercises reintroduced. Always follow your surgeon's specific guidance, as individual circumstances vary. The good news is that most athletes find their varicocele-related symptoms are substantially or completely resolved after successful surgery, often allowing better training than before.
Varicocele is the most common correctable cause of male infertility, and research suggests that intense athletic training may compound its negative effects on semen parameters. The mechanisms involve heat, oxidative stress, and mechanical factors. Importantly, these effects are often reversible: treatment of varicocele typically improves semen parameters, and temporary reduction in training intensity during conception attempts may also help. For athletes with fertility concerns, proactive assessment and management is worthwhile.
Rather than "avoid," I'd suggest being thoughtful about exercises that create high intra-abdominal pressure: heavy deadlifts, squats, leg press, and standing overhead press are the main ones. Many men can continue these with modifications (breathing technique, moderate loads, adequate rest intervals). Machine-based alternatives often allow similar muscle targeting with less pressure demand. The goal isn't necessarily to eliminate exercises, but to modify your approach so symptoms are manageable.
Post-exercise symptoms are characteristic of varicocele. During activity, blood is actively pumped through your system; once you stop, the muscular pumping ceases and blood that accumulated in the dilated veins during exercise takes time to drain. The gravitational load is now unopposed, leading to the typical dull ache or heaviness. Symptoms tend to peak 1-3 hours post-exercise and usually resolve overnight. Elevation, cool showers, and supportive underwear can help manage this pattern.
Cycling doesn't cause varicocele, but it presents specific challenges for men who have one: saddle pressure, heat accumulation, and prolonged seated positioning. The impact tends to be more on fertility (through sustained scrotal temperature elevation) than on symptoms. Good saddle choice, proper bike fit, standing intervals, and adequate ventilation can make cycling comfortable and reduce any impact. Many cyclists with varicocele continue to ride successfully with appropriate equipment modifications.
Varicocele doesn't directly affect athletic performance in the way an injury to a muscle or joint would. However, if symptoms are distracting or limiting your ability to train as you'd like, this could indirectly affect your progress and enjoyment of sport. Some men also report a psychological impact from concern about their condition. Treatment of symptomatic varicocele typically allows full return to training without limitation, often with improved comfort.
GGO Med Resources
If you'd like to explore related topics in more depth, the following pages on this website may be helpful:
Our comprehensive Varicocele Guide covers diagnosis, grading, treatment options, and what to expect from surgery or embolisation in detail. If you're considering treatment, this provides the complete picture.
The Male Fertility Overview explains the broader context of reproductive health, including how varicocele fits alongside other factors affecting fertility.
References and Further Reading
Special note about how references have been selected and used
- European Association of Urology. EAU Guidelines on Male Sexual and Reproductive Health: 2025 Update on Male Infertility. Eur Urol. 2025
