At the end of the day, my priority is your health and well-being. Whether you're dealing with a complex urological issue or seeking advice on a sensitive matter, I am here to provide the expert care you need with the compassion and understanding you deserve.
Erectile Dysfunction (ED): Causes, Diagnosis & Personalised Treatment in London
This page provides a structured, clinician-led approach to erectile dysfunction. It explains why ED happens, how physical and psychological factors interact, when investigations such as penile Doppler are useful, and how treatments are matched to the underlying mechanism. Designed for men seeking clear diagnosis, evidence-based care, and personalised treatment pathways in London.
Calm, evidence-based assessment. Clear diagnosis. Treatment matched to the actual cause—not guesswork.
Is this page for you?
This page is for you if: You're experiencing persistent difficulty getting or keeping erections firm enough for satisfying sex. You want to understand why—and what actually works—without hype, shame, or one-size-fits-all solutions.
This page is not for you if: You're looking for a quick prescription without assessment, or you believe ED is always "just psychological" or "just physical". ED is rarely that simple. The best outcomes come from proper diagnosis, not guessing.
Erectile dysfunction (ED) is common—and it can feel intensely personal. Some men notice a sudden change; others see things drift slowly over months or years. The first questions are usually the same:
Why is this happening to me?
Is it psychological or physical?
Is this "normal" or a sign of something wrong?
Am I broken—getting old—ill?
You're not alone in thinking that way. You don't need to "power through it" quietly.
I'm Mr Ollandini, Consultant Urological Surgeon in London. I help you understand what's driving your erectile dysfunction and guide you to the right pathway—without judgement, hype, or guesswork.
ED is not one condition. It's a symptom with different causes and different solutions. Many men improve with the right assessment and matched treatment.
Common pathways
How most men start
Erectile dysfunction can arise from reduced blood flow, nerve sensitivity changes, hormonal imbalance, or performance anxiety. In many men, the cause is mixed — a combination of physical and psychological factors — which is why a structured assessment works best.
Peyronie’s disease can be associated with erectile dysfunction, particularly when curvature, pain, or tissue stiffness interfere with normal erection mechanics.
his is a common and valid concern. Some treatments can affect sexual function. Traditional TURP operation or laser enucleation (HoLEP) commonly cause permanent retrograde ejaculation (dry orgasm) [53, 54], though the risk of new erectile dysfunction (ED) is relatively low (~5-10%). Medications like 5-ARIs (Finasteride) can sometimes decrease libido or cause ED. However, newer minimally invasive options like UroLift, Rezum, and potentially Aquablation are specifically designed to have a much lower impact on ejaculation and erections. It's crucial to discuss your priorities regarding sexual function when choosing a treatment.
FAQs about Erectile Dysfunction (ED): Causes, Diagnosis & Personalised Treatment in London
Understanding what's driving your ED
For many men, the first step is clarifying whether erectile dysfunction is mainly physical, psychological, or a mix—before choosing any test or treatment.
Start with a clinician-led assessment
A detailed history, examination, and targeted blood tests often point us in the right direction. Many men improve with correct first-line treatment.
Objective data when it changes decisions
When symptoms persist or treatment trials fail, investigations like penile Doppler ultrasound can help—so we avoid treating the wrong mechanism.
When to seek urgent help
If you have chest pain, severe breathlessness, fainting, or stroke symptoms, seek urgent medical help. Erectile dysfunction can sit alongside cardiovascular risk.
What ED is (and what it isn't)
Erectile dysfunction means a persistent difficulty getting or keeping an erection firm enough for satisfactory sex. It doesn't mean "zero erections ever". It doesn't mean "low testosterone". And it doesn't mean "it's all in your head".
Occasional difficulty can happen to anyone—fatigue, stress, alcohol, distraction, conflict. Erectile dysfunction is the pattern that repeats.
A quick normaliser (that still takes you seriously)
Erectile dysfunction is a symptom, not a personality flaw. It's also not a moral verdict on your relationship, your desire, or your masculinity. In medicine, it's a sign that something in the erection system—brain, nerves, hormones, blood flow, tissue response, context—isn't lining up reliably.
Once we identify which part is limiting you, choices become clearer. And many men can improve once we get the setup right.
Why erectile dysfunction happens
Most erectile dysfunction is multifactorial. You can have a physical driver and a psychological amplifier—and both deserve attention. The goal isn't to "pick a team". It's to build a plan that works.
What we assess
Common drivers we look for
Blood flow (vascular erectile dysfunction)
Reduced inflow (arterial issues) and/or poor trapping of blood (veno-occlusive dysfunction). Risk factors include smoking, diabetes, high blood pressure, and high cholesterol.
Nerves (neurogenic ED)
Diabetes, pelvic surgery, spinal issues, and some neurological conditions can disrupt signalling.
Hormones (hormonal erectile dysfunction)
Low testosterone can reduce libido and contribute to ED in some men—but it's not the default explanation. Blood tests matter.
Medication & substances
Some antidepressants, blood pressure tablets, and other medications can contribute to erectile dysfunction. Alcohol and recreational drugs can as well.
Psychological & relational factors
Performance anxiety, stress, depression, porn-related arousal mismatch, and relationship strain can all play a role. This is physiology: your brain is part of the sexual response.
Penile structure (structural ED)
Pain, curvature, or Peyronie's disease can make erections unreliable or less satisfying.
The Science of Erections: Your Body's Remarkable Mechanism
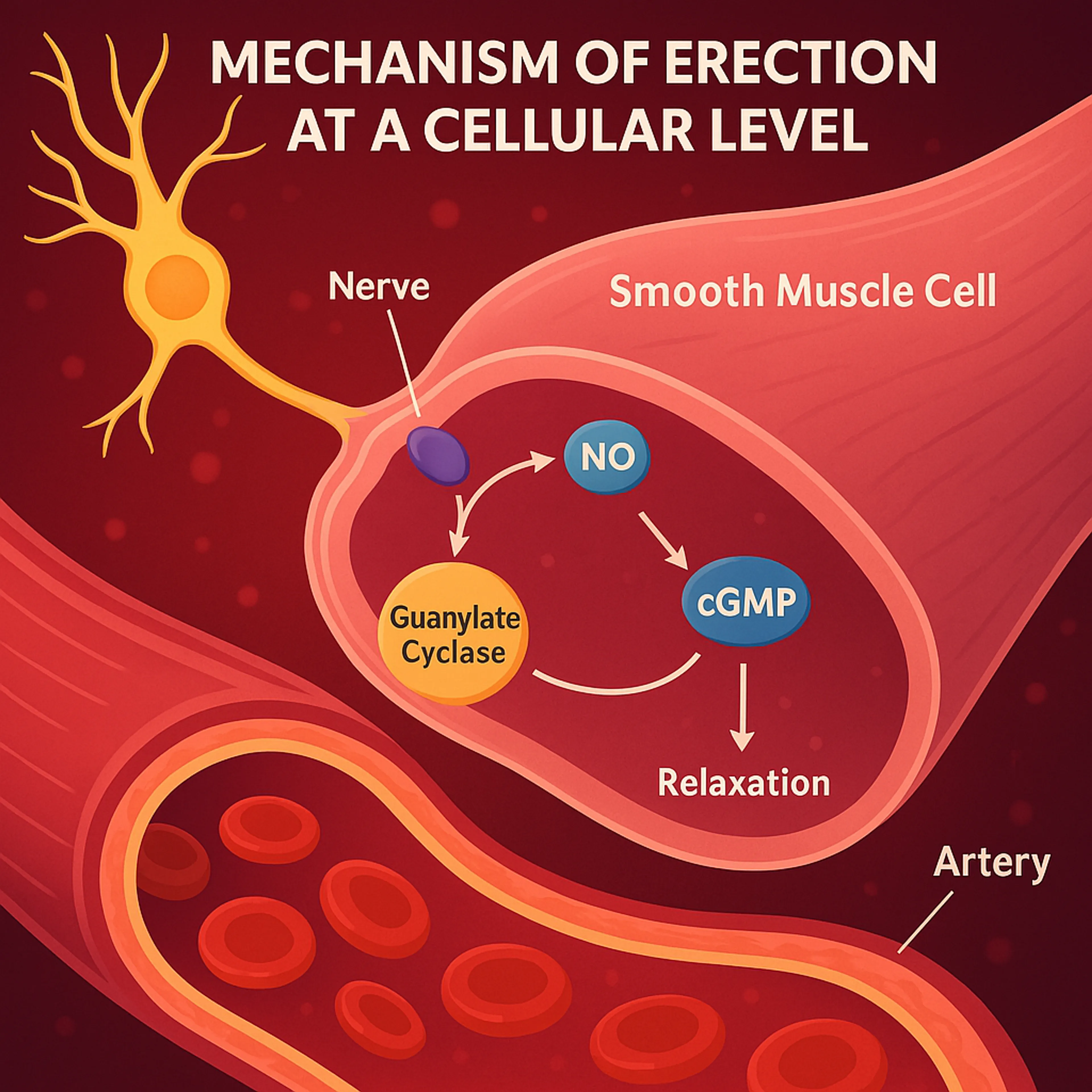
Achieving an erection is a sophisticated interplay involving the brain, nerves, hormones (like testosterone), and crucial vascular events within the penis. Triggered by arousal, nerve signals release Nitric Oxide (NO), leading to smooth muscle relaxation, increased blood flow into the erectile chambers (corpora cavernosa), and trapping of this blood (veno-occlusion) to create rigidity.
The Neuro-Vascular Cascade: A Detailed Look
Understanding the normal physiological process is fundamental to appreciating the diverse potential causes of erectile dysfunction. It's a cascade involving multiple systems:
Central Arousal (The Brain's Role): It begins with sexual stimuli – visual, tactile, auditory, olfactory, or fantasy. These stimuli are processed in specific brain areas, leading to the activation of neural pathways associated with sexual response. Libido, influenced by hormones like testosterone, plays a key role in initiating this central drive.
Neural Transmission (Nerve Pathways): The brain sends signals down the spinal cord to autonomic nerves (primarily parasympathetic nerves originating from the sacral region S2-S4) that travel to the penis. These are the pro-erectile nerves.
Peripheral Neurotransmitter Release (Nitric Oxide - The Master Key): Upon arrival at the penis, these nerve endings release crucial neurotransmitters directly onto the smooth muscle cells of the penile arteries and the corpora cavernosa. The most important of these is Nitric Oxide (NO). Additionally, the endothelial cells (the lining of the blood vessels) also release NO in response to increased blood flow shear stress. This dual source ensures a robust NO signal. The significance of NO in erection science underpins much research and treatment development. (Note: While fundamental internally, consuming external NO supplements has not been scientifically validated as an effective ED treatment UK).
Second Messenger Activation (cGMP Signal Amplification): NO diffuses into the smooth muscle cells and activates an enzyme called guanylate cyclase. This enzyme converts Guanosine Triphosphate (GTP) into cyclic Guanosine Monophosphate (cGMP). cGMP acts as a crucial intracellular second messenger, amplifying the relaxation signal.
Smooth Muscle Relaxation & Vasodilation (Opening the Floodgates): The rise in intracellular cGMP levels triggers a series of biochemical events that ultimately lead to a decrease in intracellular calcium levels within the smooth muscle cells. Reduced calcium causes these muscles (which are normally tonically contracted, limiting blood flow) to relax. This relaxation occurs in:
The walls of the small arteries (helicine arteries) supplying the penis, causing them to widen dramatically (vasodilation).
The smooth muscle tissue (trabeculae) within the corpora cavernosa themselves, allowing these spongy chambers to expand and accommodate incoming blood.
This results in a massive increase in arterial blood inflow.
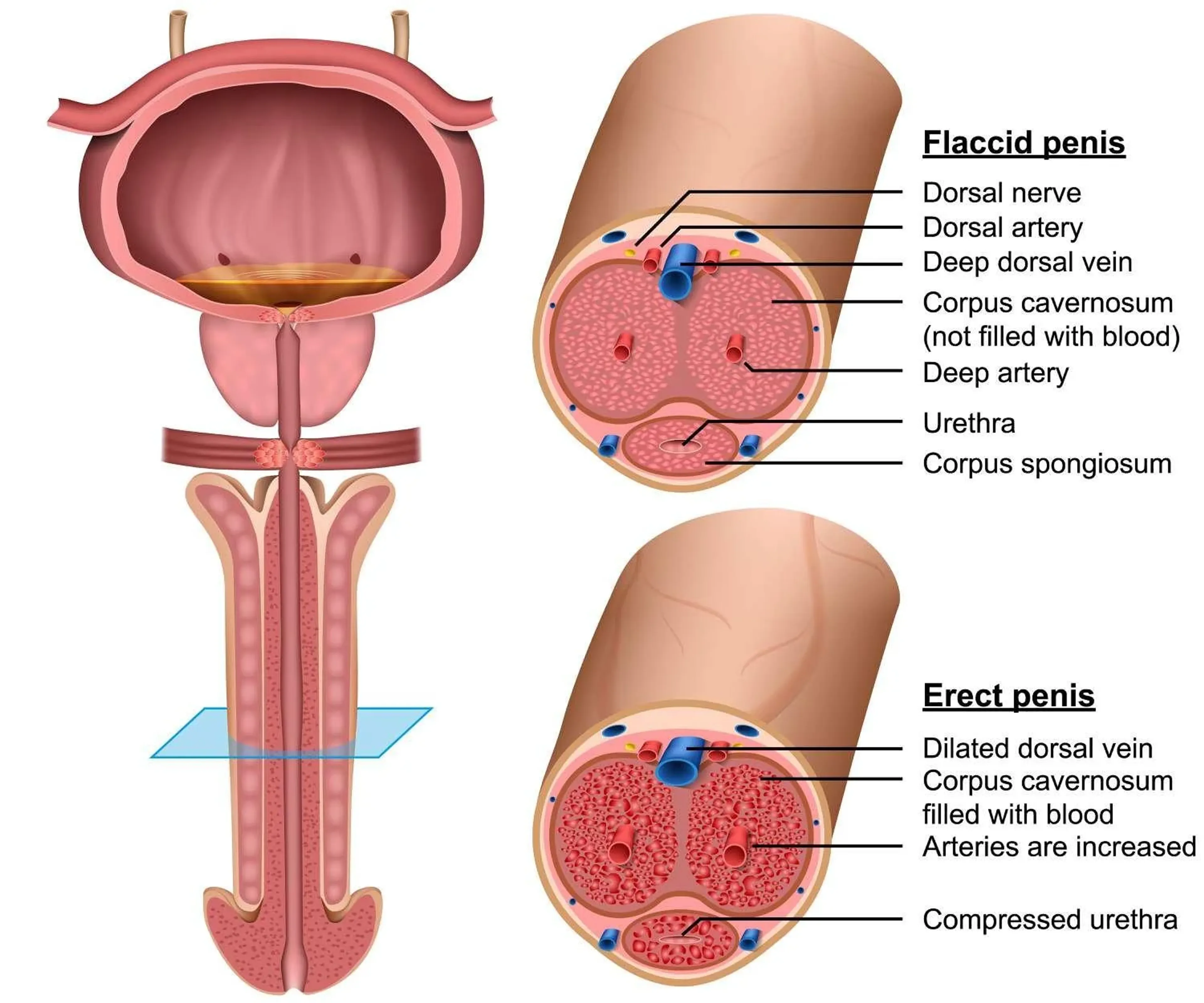
Veno-Occlusion (Trapping the Blood): As the corpora cavernosa rapidly fill with blood and expand due to the arterial inflow and smooth muscle relaxation, they press outwards against the relatively inelastic fibrous outer sheath called the tunica albuginea. This expansion physically compresses the small subtunical venules (veins) that pass through the tunica, pinching them closed. This mechanism effectively blocks the outflow of blood from the penis.
Rigidity and Maintenance (The Result): The combination of high arterial inflow and drastically reduced venous outflow causes the pressure inside the corpora cavernosa to rise significantly (intra-cavernosal pressure), leading to penile engorgement, elongation, and ultimately, full rigidity suitable for intercourse. Continued sexual stimulation is necessary to maintain the neural signals, NO release, and high cGMP levels needed to sustain the erection.
Detumescence (Returning to Flaccid State): When sexual stimulation ceases, or following orgasm and ejaculation, the pro-erectile nerve signals decrease. Simultaneously, sympathetic nerve activity may increase. An enzyme called Phosphodiesterase type 5 (PDE5), primarily located in penile smooth muscle, rapidly breaks down cGMP. Lower cGMP levels allow intracellular calcium to rise again, causing the smooth muscles to contract. This constricts the arteries, reducing inflow, and releases the compression on the veins, allowing blood to flow out, returning the penis to its flaccid state. (The major class of oral erectile dysfunction tablets, PDE5 inhibitors like sildenafil (Viagra) and tadalafil (Cialis), work precisely by blocking this PDE5 enzyme, keeping cGMP levels higher for longer when NO is released during stimulation).
Physical Causes of ED: Understanding the Organic Factors
Physical causes of erectile dysfunction commonly involve blood vessels (vascular disease—the most frequent cause, including arterial insufficiency or venous leak), nerve pathways (neurological disorders or injury), hormone levels (like low testosterone), medication side effects, or structural penile problems like Peyronie's disease. These causes often develop gradually.
Physical causes of Erectile Dysfunction
While psychological factors can certainly cause ED, particularly in younger men, underlying physical or organic problems are the primary driver in a large proportion of cases, especially as men age. These causes often develop progressively over time.
What is the main physical cause of erectile dysfunction?
By far the most common physical cause of ED, particularly affecting men over 50, is vascular disease. This umbrella term covers problems related to blood circulation within the penis. The two main vascular mechanisms are:
Arterial Insufficiency:Reduced blood flow *into* the penis, typically due to narrowing or hardening of the penile arteries (atherosclerosis), mirroring processes often occurring elsewhere in the body (like coronary artery disease).
Veno-occlusive Dysfunction (Venous Leak):An inability to properly trap blood *within* the penis during erection, leading to loss of rigidity.
While vascular issues are dominant, neurological disorders, hormonal imbalances, medication side effects, and structural problems are also significant contributors, frequently interacting with each other. A comprehensive ED diagnosis, potentially involving tests like a Penile Doppler Ultrasound, is essential to identify the specific contributors.
Physical causes of ED: a deep dive
Healthy blood flow is paramount for erections. Conditions damaging blood vessels are major culprits:
Atherosclerosis ('Hardening of the Arteries'): The build-up of fatty plaques inside artery walls restricts blood flow. This is the same process that causes heart attacks and strokes, but it often affects the smaller penile arteries earlier. Key risk factors include high cholesterol, smoking, diabetes, and hypertension.
Hypertension (High Blood Pressure): Persistently high pressure damages the delicate lining (endothelium) of blood vessels, reducing their ability to relax and dilate, thus impairing blood inflow.
High Cholesterol (Hyperlipidaemia): Excess 'bad' cholesterol (LDL) contributes directly to plaque formation in atherosclerosis.
Diabetes Mellitus: A major cause of ED due to its dual detrimental effects: damaging small blood vessels (microangiopathy) and nerves (neuropathy). High blood sugar also impairs endothelial function (NO production).
Smoking: Nicotine is a potent vasoconstrictor (narrows blood vessels). Smoking also directly damages the endothelium and accelerates atherosclerosis.
Venous Leakage (Veno-occlusive Dysfunction): Separate from inflow problems, this is a failure of the trapping mechanism. Causes can include structural changes in the tunica albuginea (sometimes related to Peyronie's), smooth muscle dysfunction, or damage to the small veins.
Cardiovascular Disease (CVD): Conditions like coronary artery disease, peripheral artery disease, and history of heart attack or stroke are strongly associated with ED because they share the same underlying vascular pathology. ED is often considered an early marker for potential CVD.
Erections rely on intact nerve pathways from the brain and spinal cord to the penis. Damage or disease affecting these pathways can cause ED:
Central Nervous System Conditions: Diseases like Multiple Sclerosis (MS), Parkinson's disease, Alzheimer's disease, brain or spinal tumours, and stroke can disrupt the brain's signals or spinal cord pathways necessary for erection.
Spinal Cord Injury (SCI): Damage to the spinal cord often interrupts the nerve signals controlling erections, with the level and completeness of injury affecting the type and degree of dysfunction.
Peripheral Neuropathy: Damage to the peripheral nerves extending to the penis. Diabetes is the most common cause (diabetic neuropathy), but it can also result from chronic alcoholism, vitamin deficiencies (especially B12), certain infections, or toxins.
Pelvic Surgery or Radiation Injury: The cavernous nerves, responsible for erections, run very close to the prostate and rectum. Surgery for prostate cancer (radical prostatectomy), bladder cancer (radical cystectomy), or rectal cancer can inadvertently injure these nerves, even with "nerve-sparing" techniques. Radiation therapy to the pelvis can also cause delayed nerve damage and vascular injury.
While less frequent than vascular or nerve issues, hormonal problems can contribute significantly to ED, primarily by affecting libido and tissue health:
Low Testosterone (Hypogonadism / Androgen Deficiency): Testosterone is vital for sexual desire (libido) and plays a role in maintaining the health and responsiveness of erectile tissues and NO pathways. Significantly low levels can make achieving erections harder, often alongside reduced libido. Assessment involves checking specific morning blood testosterone levels.
Hyperprolactinaemia (High Prolactin): Elevated levels of the hormone prolactin (often caused by a benign pituitary gland tumour called a prolactinoma, or certain medications) can suppress testosterone production and directly inhibit dopamine pathways involved in sexual function, leading to low libido and ED.
Thyroid Disorders: Both an underactive thyroid (hypothyroidism) and an overactive thyroid (hyperthyroidism) can disrupt metabolic and hormonal balance, impacting sexual function and energy levels.
Other Endocrine Conditions: Rare conditions like Cushing's syndrome or Addison's disease can also affect sexual function.
A significant number of common prescription and over-the-counter medications list ED as a potential side effect. It's vital never to stop prescribed medication without consulting your doctor, but awareness is important. Major classes include:
Antihypertensives (Blood Pressure Drugs): Thiazide diuretics (e.g., bendroflumethiazide), beta-blockers (especially non-selective ones like propranolol), and central alpha-agonists (e.g., clonidine) are more commonly implicated. ACE inhibitors, ARBs, calcium channel blockers, and alpha-1 blockers are generally less likely to cause ED.
Antidepressants: SSRIs (e.g., fluoxetine, sertraline, paroxetine) and SNRIs (e.g., venlafaxine, duloxetine) frequently cause sexual side effects including ED, delayed ejaculation, and reduced libido. Other antidepressants like bupropion or mirtazapine may have lower rates of sexual side effects.
Antipsychotics: Both older ('typical') and newer ('atypical') antipsychotics can affect sexual function through various mechanisms, including dopamine blockade and increased prolactin.
Anti-androgens & Hormone Therapies: Drugs used to treat prostate cancer (e.g., GnRH agonists like Zoladex/Prostap, anti-androgens like bicalutamide) directly reduce testosterone levels or block its action, commonly causing ED and low libido.
5-alpha-reductase inhibitors: Used for BPH and hair loss (finasteride, dutasteride), can cause ED in a small percentage of users.
Diuretics: Some diuretics beyond thiazides (e.g., spironolactone) can also contribute.
Other Medications: Certain anti-epileptics, H2-receptor antagonists (like cimetidine, though less common now), some anti-arrhythmics, opioids, and benzodiazepines can potentially affect erectile function.
Recreational Drugs: Chronic alcohol abuse, nicotine (smoking), cannabis, opioids, amphetamines, and cocaine can all negatively impact erections through vascular, neurological, or hormonal effects.
Peyronie's Disease: Characterised by the formation of fibrous scar tissue (plaque) in the tunica albuginea. This causes penile curvature or indentation during erection, which can be painful and make intercourse difficult or impossible. The plaque can also disrupt blood flow, leading to associated ED.
Chronic Systemic Diseases: Conditions like chronic kidney disease (CKD) or severe liver disease can cause ED through multiple pathways, including hormonal changes, neuropathy, vascular issues, and medication side effects.
Obstructive Sleep Apnoea (OSA): Strong association with ED. Proposed mechanisms include intermittent hypoxia (low oxygen), endothelial dysfunction, reduced testosterone due to sleep disruption, and association with other cardiovascular risk factors like obesity and hypertension. Treating OSA can sometimes improve ED.
Pelvic Trauma: Significant injuries to the pelvis (e.g., pelvic fractures from accidents) or direct trauma to the penis or perineum can damage the crucial arteries or nerves supplying the penis, leading to immediate or delayed ED.
Understanding the potential physical contributors is the first step in the ED diagnosis process, leading towards targeted and effective erectile dysfunction treatment.
Psychological Causes of ED & Performance Anxiety: The Mind's Powerful Role
Summary: The brain plays a central role in sexual function. Psychological erectile dysfunction arises when mental or emotional factors—stress, depression, relationship issues, or performance anxiety—interfere with the signals needed for an erection, even when the physical 'plumbing' is healthy. Performance anxiety creates a vicious cycle of worry and failure.
A metaphorical model showing how stress and evolutionary survival mechanisms may drive performance anxiety and psychogenic erectile dysfunction.
While physical factors are often involved, especially as men age, the power of the mind in influencing sexual response cannot be overstated. Psychological erectile dysfunction (sometimes called psychogenic ED) occurs when mental or emotional processes disrupt the normal erectile cascade.
FAQ:Can ED be "only in my mind"?
Yes, absolutely. In cases of purely psychological ED, the physical structures—nerves, blood vessels, muscles—are capable of producing an erection. However, psychological factors intervene to prevent it. This typically happens in one of two main ways:
Inhibition of Arousal Signals:Severe stress, depression, distraction, or lack of connection can prevent the brain from sending the necessary pro-erectile signals in the first place, regardless of physical stimuli.
Activation of the Sympathetic Nervous System ('Fight-or-Flight'):This is the mechanism behind performance anxiety. Worrying about performance triggers an adrenaline surge, actively constricting penile blood vessels and tensing smooth muscles, making erection physically impossible at that moment.
Psychological ED is particularly common in younger men where underlying physical disease is less likely, but it can affect men of any age. Often, a pattern of good erections in low-pressure situations (e.g., waking erections, self-stimulation) but difficulty during attempted partner sex points strongly towards a significant psychological component.
Understanding Performance Anxiety: The 'Jaguar in the Jungle' Analogy Explained
Performance anxiety ED is perhaps the most discussed psychological cause. The 'Jaguar in the Jungle' analogy helps illustrate the powerful physiological hijack that occurs:
The "Threat": The brain perceives the sexual encounter not as pleasurable but as a performance test with a high risk of perceived failure (inability to get/keep an erection). This perception triggers an alarm signal.
The Ancient Response: This alarm activates the sympathetic nervous system – the body's innate survival mechanism designed for immediate physical threats (like facing a predator).
Physiological Shift: Adrenaline causes widespread physiological changes to prepare for fight or flight: heart rate increases, breathing quickens, senses sharpen, and crucially, blood flow is redistributed.
Blood Flow Diversion: Blood is shunted *away* from organs not essential for immediate survival (including the digestive system and the penis) and *towards* the large muscles of the limbs, heart, and brain.
Anti-Erection State: Adrenaline directly causes constriction of the penile arteries and contraction of the smooth muscle within the corpora cavernosa. This actively prevents blood inflow and traps very little blood – the physiological opposite of what's needed for an erection.
The Vicious Cycle: One episode of failure due to anxiety makes the man worry more about the next time. This increased worry makes the 'threat' seem larger, triggering an even stronger sympathetic response, making failure more likely, thus reinforcing the anxiety. This cycle can quickly become established and difficult to break without intervention.
Effectively, performance anxiety turns intimacy into a perceived survival situation, physiologically blocking the body's ability to respond sexually.
Myth Buster:"Porn caused my erectile dysfunction!"
The idea of "Porn-Induced Erectile Dysfunction" (PIED) is popular in online forums but lacks formal recognition as a distinct medical diagnosis in major classifications like DSM-5 or ICD-11. While there's no doubt excessive internet pornography consumption can correlate with sexual difficulties for *some* men, causality is complex and often debated. Potential contributing factors linked to heavy use might include:
Unrealistic Expectations:Comparing real-life partners and encounters to the often artificial and high-stimulation scenarios in porn.
Desensitisation:Requiring increasingly intense or novel stimuli for arousal, making normal intimacy seem less stimulating.
Performance Anxiety:Feeling pressure to 'perform' like actors in porn.
Associated Factors:Heavy porn use might coexist with underlying anxiety, depression, relationship issues, guilt, or low self-esteem, which are themselves established causes of ED.
It's rarely accurate to attribute ED solely to porn use without a thorough assessment exploring potential underlying physical causes (vascular, neurological, hormonal) and other psychological factors. Often, problematic porn use is a symptom or coping mechanism related to other issues, rather than the primary cause itself. A balanced approach involves evaluating all potential contributors.
Other Key Psychological Contributors to ED:
Generalised Anxiety Disorder (GAD) & Other Anxiety States: Chronic worry, panic attacks, social anxiety – high baseline levels of anxiety can easily interfere with the relaxation needed for sexual response.
Depression: Clinical depression is strongly linked to ED. Symptoms like low mood, loss of interest/pleasure (anhedonia), fatigue, feelings of worthlessness, and changes in sleep/appetite directly impact libido and erectile capacity. Furthermore, some antidepressant medications can also cause ED as a side effect (see Physical Causes).
Chronic Stress: Ongoing high levels of stress from work, finances, family responsibilities, or life events elevate cortisol and adrenaline, suppressing the parasympathetic (relaxation) response needed for erection and potentially lowering testosterone over time.
Relationship Conflict & Intimacy Issues: Lack of emotional connection, unresolved anger or resentment, poor communication, boredom, or fear of intimacy with a specific partner can profoundly inhibit sexual arousal and function, even if erections are possible in other contexts.
Past Trauma or Negative Sexual Experiences: History of sexual abuse, assault, embarrassing early experiences, or upbringing with negative messages about sex can create deep-seated psychological blocks to healthy sexual function.
Low Self-Esteem & Body Image Issues: Feeling unattractive, inadequate, or ashamed of one's body can inhibit sexual confidence and arousal.
Sexual Orientation Conflicts or Guilt: Unresolved issues or guilt surrounding sexual identity or preferences can manifest as ED.
Fear of Pregnancy or STIs: While less common as a primary cause, significant anxiety about consequences can sometimes interfere with performance.
The Interplay: Mixed ED is Common It's critically important to reiterate that ED is often multifactorial. A man might start with mild physical ED due to developing vascular disease. This physical change then triggers performance anxiety, making the ED much worse than the physical component alone would suggest. Conversely, chronic stress might contribute to both psychological ED and worsen physical factors like high blood pressure over time. Effective management often requires addressing *both* the physical and psychological contributors simultaneously.
Is it psychological or physical?
This is one of the most important reframes:
"Psychological" doesn't mean "not real". It means the nervous system is interrupting the erection process—often through anxiety, stress, distraction, or learned fear of failure.
"Physical" doesn't mean "hopeless". It means we look at blood flow, nerves, hormones, medications, and penile tissue—and treat the part that's limiting you.
Clues that anxiety may be a major driver
Strong situational pattern (e.g., works alone but not with a partner, or only in certain contexts)
Rapid onset linked to a specific event (a "bad night" that spiralled)
High performance pressure, avoidance, or panic symptoms around sex
Erections are reliable when you feel safe and unobserved, unreliable when you feel evaluated
If this resonates, psychosexual support can be genuinely transformative—especially when it's practical, structured, and shame-free.
Psychosexual support: If performance anxiety, stress, or relationship dynamics are driving the pattern—sometimes alongside medical treatment
Second-line options: Vacuum devices, injection therapy (when appropriate and with proper training)
Surgical options: Penile implants for severe ED when other treatments fail
Important: Success is reliable function + satisfaction—not a porn script. We define outcomes based on what matters to you.
This ladder assumes we understand the mechanism. If we're guessing, or if first-line treatment fails, that's when assessment—and sometimes objective testing—becomes essential.
The IIEF-5 is a brief, validated questionnaire used worldwide to quantify erectile dysfunction severity. It's not a diagnosis—it's a structured way to describe your pattern.
Important context before you score yourself: Scores shift with stress, alcohol, relationship context, mood, and expectations. We use it to track change and structure the conversation—not to label you.
Complete the IIEF-5 (2 minutes)
Your score helps structure the consultation—but it doesn't tell us why erectile dysfunction is happening. That's what assessment is for.
What IIEF-5 scores mean (and what they don't)
Scores range from 5 to 25:
22–25: No erectile dysfunction
17–21: Mild erectile dysfunction
12–16: Mild to moderate ED
8–11: Moderate erectile dysfunction
5–7: Severe erectile dysfunction
Critical point: Questionnaires tell us how much ED affects you. They don't diagnose the cause. If you want to understand the mechanism—not just the severity—that's what clinical assessment is for.
How I assess erectile dysfunction
Online "one-pill-fits-all" approaches disappoint for a reason: without diagnosis, you can end up treating the wrong problem.
In my London practice, I see erectile dysfunction every week. The pattern is rarely "one cause". Assessment clarifies what's driving your symptoms, so we can match treatment to mechanism.
Step 1: A focused, non-awkward history
Onset (sudden vs gradual), variability, and what changes the outcome
Libido, ejaculation, orgasm, penile pain/curvature, and any urinary symptoms
I will ask you about night or early morning erections
I will also ask you about erection when you do masturbation
Medications, alcohol, recreational drugs, stress, mood, and relationship context
Step 2: Examination
This covers the abdomen and genitals at minimum.
Usually brief: blood pressure, body habitus, genital examination, signs of penile plaque, and prostate assessment where indicated.
Step 3: Targeted blood tests
Often includes lipids, glucose/HbA1c, and—when indicated—hormones such as testosterone (typically before 11am, with repeat testing and additional markers like SHBG, LH, and FSH if initial results are abnormal).
Most erectile dysfunction can be managed without imaging
Many men improve once we get the basics right: addressing risk factors, optimising sleep and alcohol intake, correcting tablet use, and tackling performance pressure. We move to objective testing only when it will change decisions.
When testing helps (and when it doesn't)
The point of investigations is not to impress you with a test. It's to stop us guessing when the stakes are higher.
A penile Doppler doesn't "grade your masculinity" and it doesn't diagnose relationship issues. It helps us decide whether the main driver looks vascular and/or structural, and whether treatments aimed at blood flow are likely to work.
A Doppler is not for everyone—but it is essential before certain treatments.
When objective testing commonly adds value
You've tried first-line erectile dysfunction treatment properly and results are inconsistent or poor
ED after pelvic/prostate surgery, radiotherapy, or significant pelvic trauma
The picture is mixed and the "why" is unclear
You're considering next-step treatments where
cause matters
You want objective answers rather than reassurance alone
When testing may not add much
Clear, situational ED with strong performance anxiety features and otherwise reassuring clinical picture
Early/mild erectile dysfunction that responds well to first-line treatment
Situations where the result won't change your management choices
About penile Doppler ultrasound
A penile Doppler (usually with a medication injection to create an erection in a controlled setting) can help us assess:
Arterial inflow (how well blood gets in)
Veno-occlusive function (how well blood is trapped)
Structural features (e.g., plaque/calcification patterns in some cases)
You'll be guided throughout, with clear safety advice. The procedure typically takes 30–45 minutes.
Knowledge check
Which statement is most accurate?
Do I Need a Penile Doppler Ultrasound?
Penile Doppler Ultrasound is a very good test but for very few, selected cases. Most men with erectile dysfunction do not need imaging at the start. Tests like penile Doppler are used only when results change treatment decisions.
Testosterone is often blamed for erectile dysfunction. It helps to separate two things:
Libido (desire): testosterone can influence this strongly in some men
Erection mechanics: blood flow, nerve signalling, and penile tissue response are usually the limiting steps
Low testosterone can contribute to ED in some men—especially when libido is low—but it's not the automatic explanation. If hormones are part of the picture, we confirm with properly timed blood tests (typically before 11am, with repeat testing if initial results are abnormal, plus additional markers like SHBG, LH, and FSH as appropriate) and interpret the results in clinical context.
When to check testosterone
Low or absent libido alongside erectile dysfunction
Specific risk factors (pituitary conditions, certain medications)
Testosterone testing requires correct timing and interpretation in clinical context. Isolated low levels need confirmation and assessment of overall health before treatment.
ED and heart health
Erectile dysfunction isn't always a heart problem—but the penis is a blood-flow organ. Vascular problems can appear there before they appear elsewhere.
If ED is new and persistent, and you have cardiovascular risk factors (smoking, diabetes, high blood pressure, high cholesterol, excess weight, low activity, poor sleep), use it as a prompt to review your overall cardiovascular health. That may involve your GP as well as specialist assessment.
If you're worried ED is a sign of something serious
Erectile dysfunction can precede cardiovascular disease in some men—because the penile arteries are smaller and may show damage earlier than coronary arteries. This doesn't mean every man with ED has heart disease, but it's a reasonable prompt to check.
New erectile dysfunction with multiple cardiovascular risk factors
Reduced exercise tolerance or breathlessness on exertion
Family history of early heart disease
Abnormal blood pressure, cholesterol, or diabetes control
Assessment doesn't mean panic—it means being sensible. Many men use ED assessment as a prompt to improve overall health, which benefits more than just sexual function.
Medications that can contribute to erectile dysfunction
Several common medications can affect erectile function. That doesn't mean they're wrong for you—it means we need to weigh benefits against side effects, and sometimes adjust treatment.
Critical: Don't stop medications without medical advice. Some conditions require continuous treatment. Stopping suddenly can be dangerous.
Common medication categories that may contribute to ED:
Antidepressants: Particularly SSRIs and SNRIs (e.g., sertraline, citalopram, venlafaxine)
Antihypertensives: Some blood pressure tablets, particularly older beta-blockers and thiazide diuretics
5-alpha reductase inhibitors: Finasteride, dutasteride (used for prostate enlargement or hair loss)
Opioid painkillers: Long-term use can affect hormone levels and sexual function
Antipsychotics: Can affect dopamine and prolactin levels
H2 antagonists: Cimetidine and similar medications for acid reflux (less common with newer PPIs)
If you suspect a medication is contributing, discuss it with your prescribing doctor. There are often alternatives or additional treatments that allow you to manage erectile dysfunction while continuing necessary medication.
Many men worry that their medication is causing erectile dysfunction. While certain drugs can contribute, in many cases ED is linked to the health condition being treated, rather than the medication itself.
Treatment options (detailed)
Several effective treatment options exist. The key is matching the right tool to the right mechanism—and being honest about what we do and don't know.
Cardiovascular Health Focus: Since vascular disease is the most common cause, managing risk factors is key: controlling blood pressure, diabetes, and cholesterol levels; stopping smoking; maintaining a healthy weight; and regular aerobic exercise [Ref 5, 14].
Dietary Changes: Emphasising a diet rich in fruits, vegetables, whole grains, fish, and nuts (like the Mediterranean diet) and low in red/processed meats, refined grains, and sugary drinks supports endothelial health and blood flow.
Exercise: Regular moderate-to-vigorous aerobic exercise has been shown to improve erectile function, likely by improving blood flow, endothelial function, and reducing cardiovascular risk.
Weight Loss: For overweight or obese men, losing weight can improve testosterone levels, insulin sensitivity, and vascular health.
Smoking Cessation: Quitting smoking provides rapid and significant benefits to vascular health.
Alcohol Moderation: Reducing excessive alcohol intake is important for nerve function and overall health.
Stress Reduction & Sleep: Managing chronic stress and ensuring adequate sleep quality can positively impact hormonal balance and autonomic nervous system function.
PDE5 inhibitors (e.g., sildenafil/Viagra, tadalafil/Cialis): effective for many men with erectile dysfunction, but not magic—dose, timing, stimulation, and expectations matter
Phosphodiesterase type 5 inhibitors (PDE5i) are the most commonly prescribed medical treatment for ED and have revolutionized management since their introduction. They are effective for many men, particularly those with mild to moderate ED, or ED related to psychogenic causes or mild vascular issues.
Mechanism of Action: They block the PDE5 enzyme in the penis, preventing the breakdown of cGMP. This allows cGMP levels to build up in response to sexual stimulation and NO release, promoting smooth muscle relaxation, increased blood inflow, and firmer, longer-lasting erections. They require sexual stimulation to be effective.
Available Options in the UK:
Sildenafil (Viagra, Viagra Connect): The first PDE5i. Onset typically 30-60 minutes, duration about 4-5 hours. Absorption can be delayed by high-fat meals. Viagra Connect is available OTC after pharmacist assessment.
Tadalafil (Cialis, Cialis Daily): Characterised by a much longer duration of action (up to 36 hours), offering greater spontaneity ("the weekend pill"). Absorption is not significantly affected by food. Available as 'on-demand' doses (10mg, 20mg) or a low daily dose (2.5mg, 5mg) for continuous effect.
Vardenafil (Levitra): Similar profile to sildenafil (onset ~30 mins, duration 4-5 hours). Some men may respond better to vardenafil if sildenafil is ineffective. Food effect similar to sildenafil.
Avanafil (Spedra): A newer generation PDE5i with potentially faster onset (15-30 minutes for some) and similar duration to sildenafil/vardenafil. May have slightly higher selectivity for PDE5, potentially reducing some side effects.
Efficacy: Success rates are generally 60-80%, depending on the cause and severity of ED. Less effective in severe vascular disease, significant nerve damage (e.g., post-prostatectomy), or severe diabetes.
Clinical Pearls & Patient Guidance:
Multiple Trials Needed: Don't give up after one try. It often takes 4-8 attempts with adequate stimulation to determine if a specific PDE5i at an optimal dose works for you.
Timing is Key: Take the medication appropriately before anticipated sexual activity (allowing for onset time).
Stimulation is Required: These drugs enhance a natural response; they don't create desire or erections without arousal.
Side Effects: Common side effects are usually mild and transient, including headache, facial flushing, nasal congestion, indigestion, and occasionally visual disturbances (blue tinge - sildenafil) or back/muscle pain (tadalafil).
Safety and Contraindications: The primary contraindication is concurrent use of nitrates. Caution is needed with certain heart conditions and with alpha-blocker medications for BPH (potential for low blood pressure). A prescription requires a prior medical assessment.
Psychosexual support when anxiety, stress, shame, avoidance, or relationship dynamics are central (sometimes alongside medical treatment)
How to avoid 'false failures' with tablets
They usually require sexual stimulation; they don't create desire on their own
Timing and dose matter (and vary between medications—sildenafil typically 1 hour before, tadalafil can be daily or on-demand)
Alcohol, fatigue, stress, and distraction can override the effect
If you tried them once, at the wrong time, under pressure—your result may not reflect true response
In my practice, a significant proportion of "tablet failure" becomes "tablet success" once we correct the setup—or we learn that another pathway is more appropriate.
When first-line isn't enough
Vacuum erection devices
(mechanical option; some couples find them helpful, some don't—worth trying before more invasive options)
Intracavernosal injection therapy
(highly effective in selected men; requires safe teaching and clear discussion of risks including priapism)
Penile implants
(a reliable surgical option for severe erectile dysfunction when other treatments fail; involves surgery and irreversible change)
About 'regenerative' or device-led treatments
You'll see a lot online about low-intensity shockwave therapy (Li-ESWT) and other interventions. Research is evolving. Some men report benefit; others don't.
The responsible approach is to discuss the evidence quality, your goals, your baseline vascular status, and whether objective testing (like Doppler) should come first—so we avoid paying for the wrong treatment for the wrong mechanism.
Common side effects include headache, flushing, indigestion, and nasal congestion. They are not suitable with certain heart medications (especially nitrates used for angina). We check your medical history and current medications before prescribing erectile dysfunction treatment.
Can cause pain, bruising, and rarely a prolonged erection (priapism), which needs urgent treatment. Proper training and dose titration reduce risks significantly. Not suitable for all men—requires assessment and supervised initial use.
Surgery carries risks including infection, mechanical failure over time, and revision surgery. Modern devices have good reliability, but this is an irreversible change that requires careful decision-making. We only recommend this when other erectile dysfunction treatments have genuinely failed.
Erectile dysfunction is treatable. The best outcomes come from matching treatment to mechanism. If "trying another pill" isn't good enough, structured assessment is the difference between guessing and choosing well.