


A man comes in holding a sheet of paper and bad news he has given himself.
A laboratory — one he found on his own — has reported his sperm morphology at 2%, with a line at the bottom advising him to see an andrologist urgently. He and his partner have been trying for three months. He has read the word “urgently”, he has read “2%”, and he has spent two weeks quietly certain he is the reason they have no child.
Here are the rest of his numbers, the ones he skipped past. Sperm concentration: 530 million per millilitre. Motility: 51% swimming forward. Volume: 3.2 millilitres. Every one of those is not merely normal but excellent — the concentration alone is more than thirty times the reference figure. The single value below range was the morphology. And three months of trying is not, by any medical definition, infertility.
The only thing wrong with this man was the fear he had been handed.
I want to be careful here, because this cuts both ways. The lesson is not “ignore the low number”. The lesson is that a semen analysis is a professional document wearing a friendly disguise. It hands you tidy figures and a “normal range” column, and it looks as though you can read it. You can read the words. What you usually cannot do safely is interpret what they mean in context — and neither can an automated lab comment, without the whole clinical picture. A single number, out of context, means very little. The whole picture means almost everything.
So this page is not here to teach you to diagnose yourself. Quite the opposite. It is here to show you why the report is so easy to misread, what the numbers actually are, and why the sensible move is to do the test and then put it in front of someone whose job is reading them. That part is mine.
Trying for under a year? That is not yet what doctors mean by infertility — the usual definition is twelve months of regular, unprotected sex. It is completely reasonable to get checked sooner, especially if something worries you. Just don’t read an early result as a verdict.
What a semen analysis actually measures
A semen analysis looks at a single sample under strict laboratory conditions and reports a handful of measurements. They sound self-explanatory. They are not quite. Here is what each one actually is — and, just as importantly, what it is not.
The four main measures
What the numbers mean
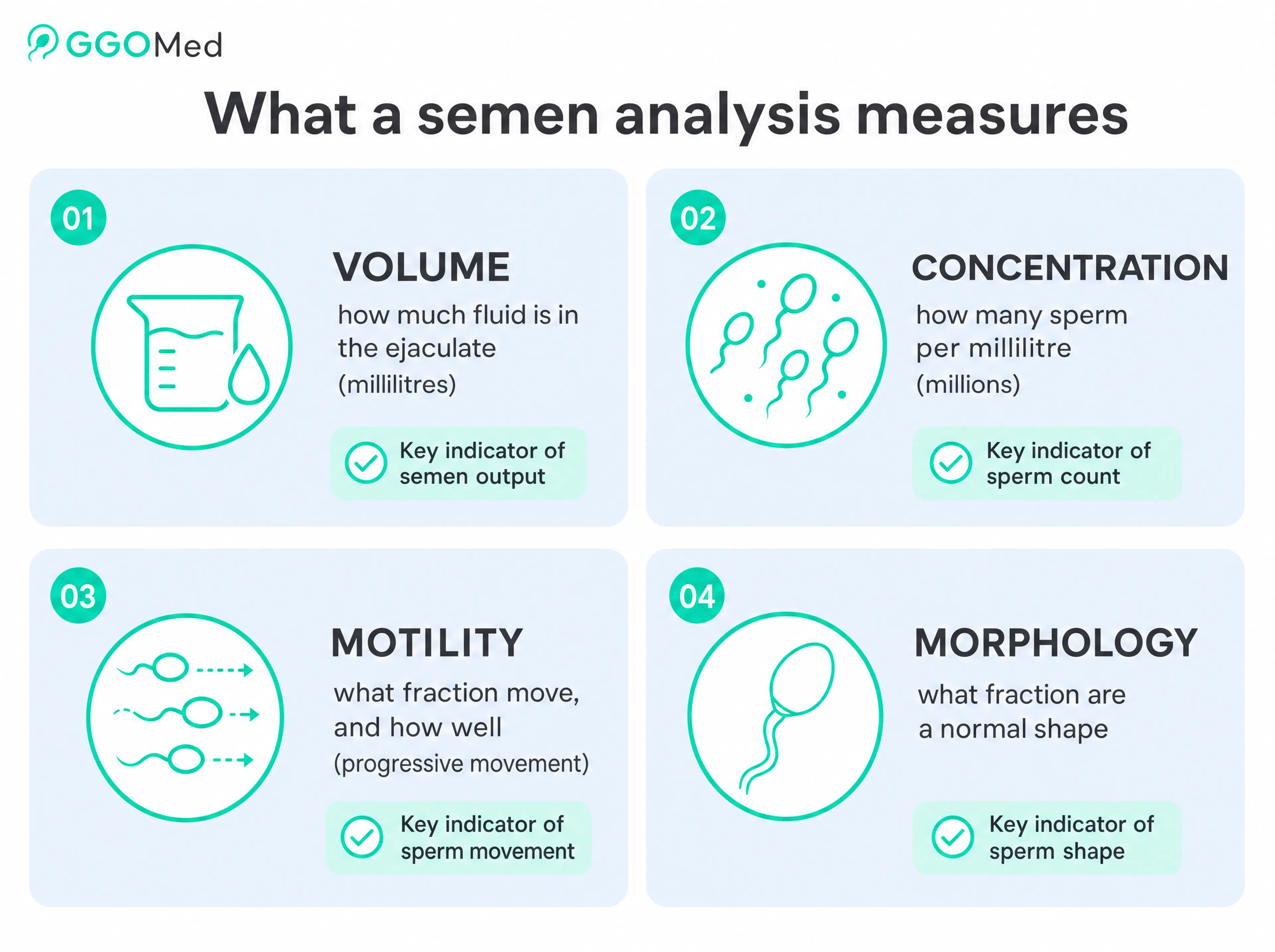
Volume
How much fluid is in the ejaculate, in millilitres — mostly fluid from the prostate and seminal vesicles, not sperm. A low volume can point to a collection or blockage issue, not necessarily anything wrong with the sperm themselves.
Concentration
How many sperm there are per millilitre, in millions. This is the figure people fixate on, and it genuinely matters — but “how many” is not the same as “how well they work”.
Motility
What fraction of the sperm move, and how well. Progressive motility — swimming purposefully forward — matters most for natural conception. A sample can be crowded yet sluggish, or modest in number yet brisk.
Morphology
What fraction of the sperm are a “normal” shape, against strict criteria. This is the single most misunderstood figure on the report — and the next section is largely about why.
There is usually a fifth line — vitality — measuring how many sperm are alive, which matters mainly when motility is very low. Beyond these, more specialised tests exist, such as DNA fragmentation, and those come up later — because they are exactly the kind of thing the standard report does not show you.
The thing to hold on to: each line measures a different thing, and no single line is “the result”. A report is a small panel of related clues, not a verdict with a headline number.
The trap of the “normal range”
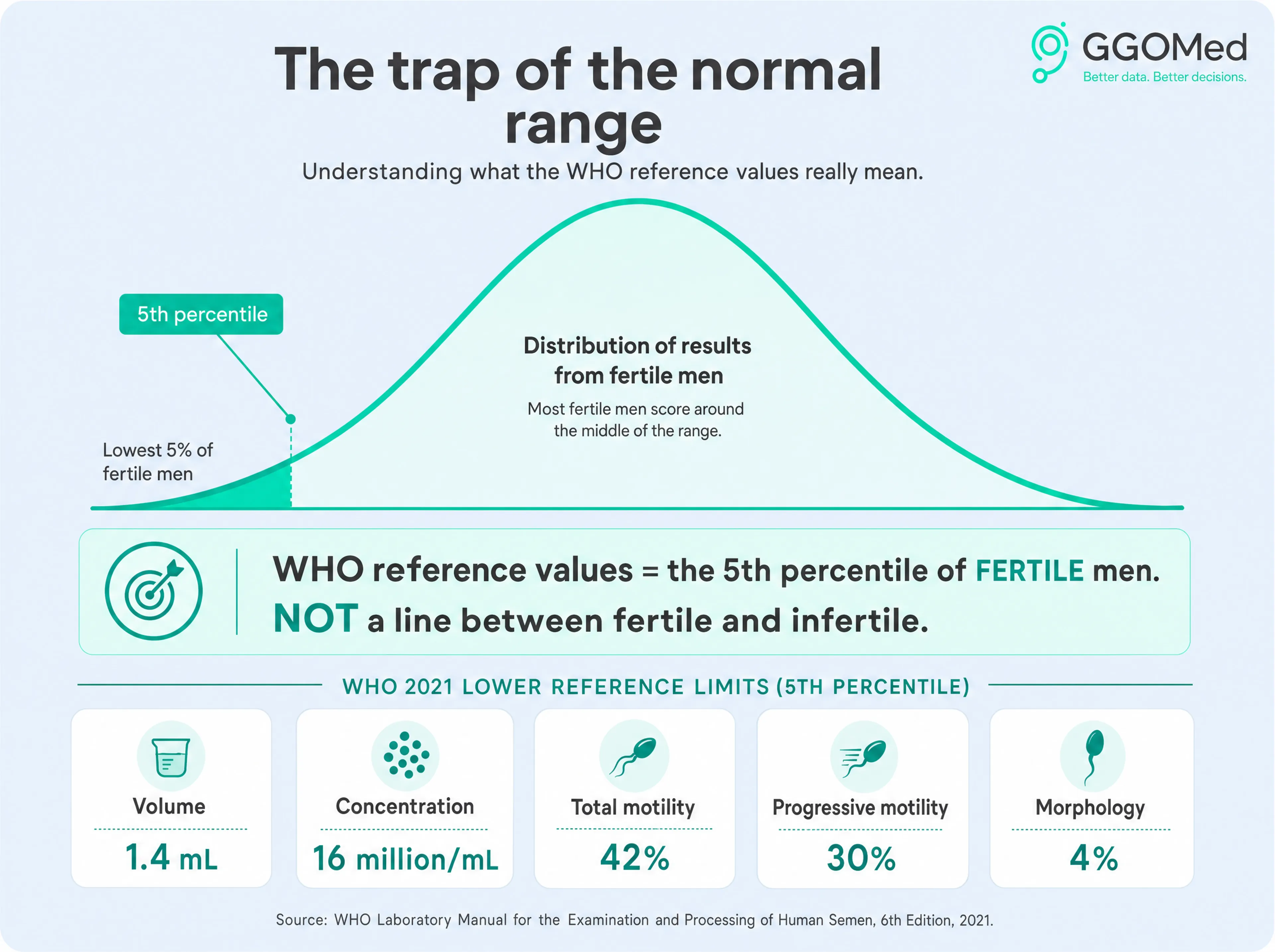
Look at the right-hand column of almost any semen analysis and you will see a “reference range” or “normal value” next to each result. It is the most reassuring-looking part of the page, and the most misleading.
Here is what those values actually are. The World Health Organization publishes them — the current set is from the 2021 sixth edition — and they are drawn from the 5th percentile of a large group of men who fathered a child naturally, their partners conceiving within twelve months. In plain terms: they took several thousand men known to be fertile, lined up their results, and the reference figure is roughly the value below which only the lowest 5% of those fertile men fell. So the “normal range” is not a line between fertile and infertile — it is a description of where fertile men sit. The WHO itself says exactly this: its manual states the 5th percentile does not represent a cut-off between fertile and infertile, and many specialists argue the equation “below the threshold = infertile” should be abandoned outright.
The clearest example is morphology, and it catches almost everyone.
Knowledge check
A semen analysis reports 4% normal sperm morphology. What does that mean?

That is the friendly disguise in a single figure. “4% normal” sounds like catastrophe; it is the ordinary benchmark. So when the man at the top of this page saw 2%, flagged in red, he read it as the end of his chances — when in a sample with 530 million sperm per millilitre and brisk motility, an isolated low morphology is, on its own, very weak evidence of anything.
I want to be precise, because this is where it would be easy to over-correct: I am not telling you morphology is meaningless. A genuinely abnormal morphology — low, persistent across repeated tests, and sitting alongside other abnormal parameters — can matter. The point is the opposite of dismissive: deciding whether a number matters is not a job you can do from the page. An isolated figure, flagged by a system with no view of the whole, is not a diagnosis.
The one thing to take from this section
A result below the “normal range” does not mean you are infertile, and a result inside it does not guarantee anything. The range describes fertile men; it does not sort people into fertile and infertile. That sorting — if it is needed at all — takes context, repetition, and a trained read.
Why a single result tells you so little
Even setting aside how the numbers are interpreted, there is a deeper problem with treating one report as the truth: the same man can produce strikingly different results from one sample to the next. A semen analysis is a snapshot of a moving target.
Two things drive this. First, sperm take roughly two to three months to make — the production cycle is about 72 to 74 days. So a sample taken today reflects what your body was doing two or three months ago: a fever, a heavy work stretch, a bad bout of stress, even a viral illness, can show up in a result long after you have forgotten it. The number on the page is a postcard from the recent past, not a permanent verdict.
Second — and this surprises almost everyone — how many days you abstain before the test changes the numbers. The WHO asks for two to seven days of abstinence precisely because the figures move with it.
Two things the report won't tell you
Myth
Myth: My result is my result — it is a fixed fact about me.
Fact
Fact: The same man, tested after two days versus seven days of abstinence, can show meaningfully different volume, concentration, motility and even DNA quality. Longer abstinence tends to raise volume and count but can worsen motility and DNA integrity; shorter abstinence does the reverse. The test has conditions for a reason.
Myth
Myth: One abnormal semen analysis means there is a problem.
Fact
Fact: A single off result, on its own, often means very little. Because of natural variation and the long production cycle, an abnormal finding is repeated — usually a few weeks to a couple of months later — before anyone should read anything into it.
This is why, when a result comes back abnormal, the right next step is almost never panic — it is a repeat test under proper conditions, and a conversation about everything that might have nudged the first one. A single result is a starting point, not a finishing line.
Fertility is a probability, not a verdict
Even a careful, repeated, well-conducted semen analysis cannot do the one thing people most want it to do: tell you, yes or no, whether you can father a child. That is not a limitation of the test. It is the nature of fertility.
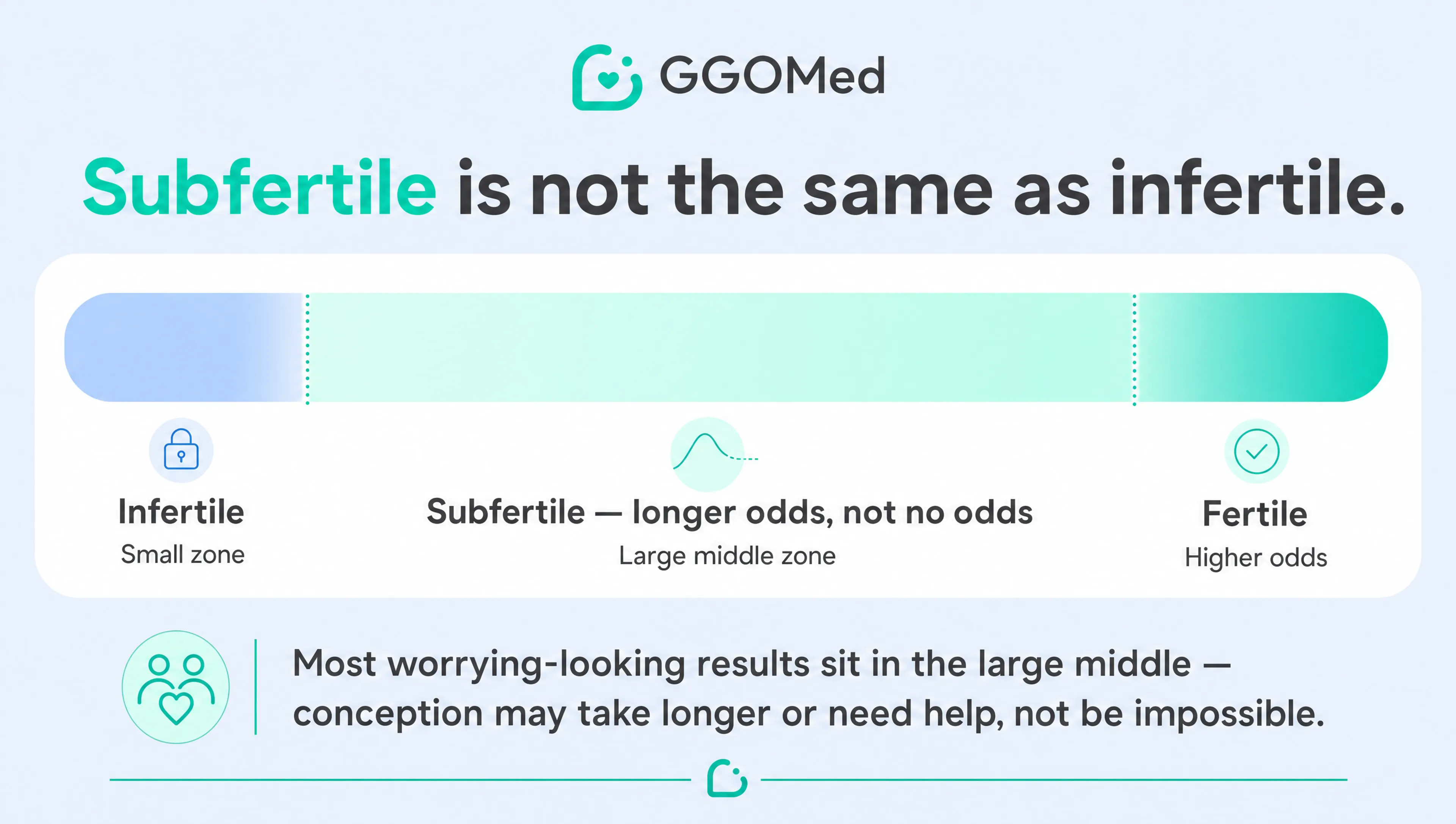
Fertility is not a switch — on or off, fertile or not. It is a probability, a likelihood of conception over time, and the numbers shift that likelihood up or down rather than settling it. A result below the reference range lowers the odds; it does not abolish them. Men with figures well under the WHO values do father children, sometimes easily. A result inside the range raises the odds; it does not guarantee them. There is a word for the large middle ground this creates — subfertile, meaning conception may take longer or need some help, which is a very different thing from infertile, meaning it cannot happen without intervention. Most men who get worried results are nearer the first than the second.
And there is one more reason the report can never be a verdict on its own: it only describes one half of the couple. Conception is a joint event. The same male result carries entirely different weight depending on the other half of the picture — a borderline figure alongside a straightforward female assessment is not the same situation as the identical figure alongside other factors. The female reproductive assessment sits outside my direct practice, so I will not pretend to interpret it — but any honest reading of a man’s result keeps it in view, because he is one half of a pair, not a problem to be solved in isolation.
“Subfertile” and “infertile” are not the same word. Most worrying-looking results sit in the subfertile range — longer odds, not no odds. Which one applies to you is exactly the kind of judgement that needs a professional and the whole picture, not a glance at one column.
When the numbers look normal but something still is not right
So far this page has been about not panicking over numbers that look bad. Here is the other edge of the same blade: sometimes the numbers look good, and something is still wrong.
A standard semen analysis counts sperm, watches them swim, and checks their shape. What it does not do is look inside them — at whether the genetic material they carry is intact. Sperm can be plentiful, fast and well-formed on paper, yet carry a high level of DNA damage that a conventional report will never reveal. This is measured by a separate test — sperm DNA fragmentation — and it is one of the clearest reasons a “normal” result does not always close the case.
I will not unpack the whole topic here, because it belongs to a fuller discussion — particularly around varicoceles, which are one of the common drivers of this kind of hidden damage. The reason it sits on this page at all is to make a single point: a reassuring standard report is not always the end of the story, and knowing when to look further is precisely the part you cannot do from the page yourself. It takes someone who knows which normal-looking result still deserves a second, deeper look.
Varicocele and fertility: when good numbers hide a problem
How a varicocele can damage sperm DNA even when the standard analysis looks normal — and when that is worth investigating.
The bottom line: do the test, then bring it to someone who reads them
Let me bring this back to the man at the top of the page, because his story holds the whole argument in miniature. His report looked readable. It had numbers, percentages, a tidy “normal range”. One figure was flagged, he read it alone, and he spent two weeks in fear — over an isolated value, in an excellent sample, after three months of trying. Nothing was wrong except the reading.
So here is what I would actually want you to take away:
- The “normal range” describes fertile men — it is not a line between fertile and infertile.
- A single number, out of context, means very little.
- A single test, without a repeat, is a snapshot, not a verdict.
- Fertility is a probability shared between two people, not a yes/no stamped on one sheet.
None of that means the test is not worth doing. It absolutely is — a semen analysis is one of the most useful first steps in understanding fertility, and I would never tell anyone to skip it. The point is simpler, and I think kinder: do the test — and then do not try to read it alone. That is not a failing on your part. Reading these reports in context, knowing what to repeat, what to ignore, and what deserves a deeper look, is a clinical skill. It is mine, and I am glad to put it to work for you.
Need a semen analysis — or trying to make sense of one you've already had?
I arrange testing through accredited laboratories and read the results with you, in context, not in panic. If you have a report that worried you, bring it.
Related reading
Struggling to conceive: the male side
Where a semen analysis fits among the other parts of a male fertility assessment.
Varicocele and fertility
One of the most common — and correctable — causes of male fertility problems.
Testosterone and fertility
Why taking testosterone can quietly switch off your own sperm production.
