

Blood in your urine — haematuria — is always worth investigating. In most cases the cause is benign and treatable. But because a small number of cases point to something more serious, every episode deserves a proper assessment. This guide explains what haematuria means, what causes it, and exactly what to expect from the diagnostic process.
Worried after seeing blood in your urine?
Book a same-week assessment. We'll take it seriously, move quickly, and explain everything clearly.
1. What Is Haematuria?
Haematuria means blood in the urine. It is a sign — not a diagnosis — indicating that bleeding is occurring somewhere along the urinary tract, from the kidneys down to the urethra. Understanding the type of haematuria you have helps guide the right investigations.
Three Types of Haematuria
Macroscopic (Visible)
Urine appears pink, red, or cola-coloured. Blood clots may be present. Even a single episode — painless or not — requires urgent investigation. Visible haematuria carries a higher risk of underlying malignancy and triggers the NHS 2-week-wait cancer referral pathway.
Microscopic (Non-Visible)
Blood is only detectable on urine dipstick or microscopy (≥3 red blood cells per high-power field). Often found incidentally. Still requires investigation — the absence of visible blood does not mean the cause is benign.
Glomerular vs Non-Glomerular
Glomerular bleeding originates in the kidney filters and is suggested by dysmorphic red cells, red cell casts, or significant proteinuria on urine microscopy. Non-glomerular bleeding arises from the urological tract (ureter, bladder, urethra, prostate). This distinction guides whether urology or nephrology leads the investigation.
Key Points
- Haematuria is a sign, not a diagnosis
- Visible haematuria carries higher malignancy risk and triggers urgent referral
- Microscopic haematuria still requires full investigation
- Urine microscopy helps distinguish glomerular from urological bleeding
- Understanding the type guides the right investigations from the start
2. Potential Causes
Haematuria has a wide range of causes — from entirely benign conditions to serious pathology. The most important principle: the cause is never assumed. Every case is investigated systematically.
Overview of Cause Categories
Common Benign Causes
UTIs, kidney and bladder stones, benign prostatic hyperplasia (BPH), and prostatitis account for the majority of haematuria cases. These are treatable — but visible haematuria still requires investigation even after a UTI has resolved.
Urological Cancers
Bladder cancer is the most common malignancy presenting with visible haematuria. Kidney cancer (RCC), upper tract urothelial carcinoma (UTUC), and — rarely — prostate cancer are also in the differential. Painless visible haematuria is the classic presentation of bladder cancer.
Kidney (Glomerular) Disease
IgA nephropathy, Alport syndrome, thin basement membrane disease, and post-infectious glomerulonephritis can all cause haematuria. These are managed by nephrology, not urology. Urine microscopy findings (casts, dysmorphic RBCs, proteinuria) point in this direction.
Other Important Causes
Trauma, anticoagulant medications (warfarin, apixaban, rivaroxaban), strenuous exercise, inherited conditions (polycystic kidney disease, sickle cell), and idiopathic haematuria. Important: anticoagulants do not explain haematuria — investigation is still required.
Urinary Tract Infections (UTIs): Dysuria, frequency, urgency, and lower abdominal discomfort are typical. Fever suggests upper tract (kidney) involvement. Important: visible haematuria in the context of a UTI still requires investigation after treatment to confirm resolution.
Kidney and Bladder Stones: Renal colic — colicky pain radiating from loin to groin — is characteristic. Haematuria occurs as stones scrape the urothelium. Nausea and vomiting are common. Bladder stones cause irritative lower urinary tract symptoms.
Benign Prostatic Hyperplasia (BPH): In men, an enlarged prostate can cause intermittent haematuria alongside weak stream, hesitancy, and nocturia. See our LUTS diagnosis guide and BPH surgery page for more detail.
Prostatitis: Bacterial or non-bacterial inflammation of the prostate can cause haematuria alongside pelvic pain and urinary symptoms. See our chronic pelvic pain page for related information.
Bladder Cancer: The most common malignancy presenting with haematuria. Painless visible haematuria is the classic presentation. Risk factors include smoking (the single biggest modifiable risk), age over 50, occupational exposures (aromatic amines, dyes), and pelvic radiotherapy. Read more: Smoking and Your Urological Health.
Kidney Cancer (Renal Cell Carcinoma): May present with visible or microscopic haematuria, persistent flank ache, or a palpable mass — though many are now detected incidentally on imaging.
Upper Tract Urothelial Carcinoma (UTUC): Cancer of the renal pelvis or ureter lining. Shares risk factors with bladder cancer. Can be subtle on imaging; CT urography is essential.
Prostate Cancer: Rarely causes haematuria directly — only when advanced disease invades the bladder or urethra. Raised PSA, LUTS, or bone pain are more typical presentations.
IgA Nephropathy: The most common glomerular cause of haematuria. Characteristically presents with episodes of visible haematuria during or shortly after upper respiratory tract infections.
Alport Syndrome: A genetic condition associated with progressive kidney disease and sensorineural hearing loss.
Thin Basement Membrane Disease: A benign inherited condition causing persistent microscopic haematuria, usually without progression to kidney failure.
Post-Infectious Glomerulonephritis: Follows streptococcal throat or skin infections. Typically self-limiting.
Glomerular disease is managed by nephrology. Urine microscopy findings — red cell casts, dysmorphic RBCs, significant proteinuria — are the key diagnostic clues.
Trauma: Accidents, falls, blunt abdominal or pelvic trauma, and pelvic fractures can all cause haematuria. Urgent A&E assessment is required.
Anticoagulant Medications: Warfarin, apixaban, rivaroxaban, and aspirin can unmask bleeding from an underlying lesion. Critically: anticoagulants do not explain haematuria — investigation is still required even in patients on blood thinners. Other drugs (cyclophosphamide, some antibiotics, NSAIDs) can cause bladder irritation or interstitial nephritis.
Strenuous Exercise: Long-distance running and cycling can cause temporary haematuria (visible or microscopic). This is a diagnosis of exclusion — other causes must be ruled out first.
Inherited Conditions: Polycystic kidney disease (PKD) — cysts can bleed. Sickle cell disease — affects kidney function and can cause haematuria.
Idiopathic Haematuria: No cause is found despite thorough investigation, particularly in younger patients with microscopic haematuria. Follow-up monitoring is recommended.
A note on anticoagulants: Patients on warfarin, apixaban, or rivaroxaban sometimes assume their haematuria is explained by their medication. It is not. Anticoagulants lower the threshold for bleeding from an underlying lesion — they do not create haematuria from nothing. Investigation is always required.
3. Risk Factors
Risk factors help determine how urgently haematuria needs investigating and how extensive the workup should be. No single factor is decisive — they are always considered together.
Key Risk Factors at a Glance
Age Over 50
The risk of urological malignancy rises significantly with age. Haematuria in patients over 50 is investigated more urgently, regardless of other factors.
Smoking
The single biggest modifiable risk factor for bladder cancer. Smokers and ex-smokers with haematuria are investigated as high-risk. Read: Smoking and Your Urological Health.
Visible Haematuria
Visible blood in the urine carries a higher risk of malignancy than microscopic haematuria and triggers the NHS 2-week-wait urgent cancer referral pathway.
Male Sex
Men have a higher baseline risk of bladder cancer. Haematuria in men is therefore investigated with a lower threshold for urgent referral.
Occupational Exposures
Prolonged exposure to aromatic amines (rubber, dye, textile, leather industries) significantly increases bladder cancer risk. A full occupational history is taken at assessment.
Other Factors
Pelvic radiotherapy, chronic catheterisation, certain medications (cyclophosphamide), and family history of urological or kidney disease all contribute to risk stratification.
Risk factors are never assessed in isolation. Two clinical examples illustrate how they combine:
Higher-risk scenario: A 68-year-old man, ex-smoker, presenting with a single episode of painless visible haematuria. Multiple high-risk features (age, sex, smoking history, visible haematuria) → urgent 2-week-wait referral, CT urography + flexible cystoscopy.
Lower-risk scenario: A 28-year-old woman, non-smoker, with microscopic haematuria found incidentally on a routine urine dipstick, no symptoms. Fewer risk factors → investigation still required, but the pathway may be less urgent. Urine microscopy, renal function, and blood pressure are checked first to exclude glomerular disease.
4. The Diagnostic Pathway
The haematuria diagnostic pathway is systematic and tailored to each patient. It typically involves six steps — though not every patient needs every investigation. The pathway is adapted based on risk factors, clinical findings, and results at each stage.
The assessment begins with a detailed history: when haematuria was first noticed, whether it is visible or microscopic, whether it is painful or painless, associated symptoms (dysuria, frequency, urgency, loin pain, weight loss, night sweats), and a full review of medications, occupational history, smoking history, and family history.
Physical examination includes abdominal palpation (for renal masses), digital rectal examination in men (to assess the prostate), and blood pressure measurement.
Urine Dipstick: Detects blood, protein, nitrites, and leucocytes. A positive dipstick for blood must be confirmed by microscopy — dipstick alone is not sufficient.
Urine Microscopy, Culture & Sensitivity (MC&S): Confirms the presence of red blood cells, identifies infection, and looks for casts and dysmorphic RBCs (suggesting glomerular disease).
Urine Cytology: Examination of shed cells in the urine for malignant or atypical cells. Most useful for detecting high-grade bladder cancer and carcinoma in situ (CIS). A negative cytology does not exclude cancer.
Urea & Electrolytes (U&Es) and eGFR: Assess kidney function. Essential before contrast-enhanced CT imaging.
Full Blood Count (FBC): Checks for anaemia (which may indicate chronic blood loss) and signs of infection or systemic disease.
PSA (Prostate-Specific Antigen): Offered to men as part of a shared decision-making discussion. PSA is not a perfect test — it can be elevated by BPH, prostatitis, and other factors — but it contributes to the overall clinical picture. See our LUTS diagnosis guide for more on PSA in context.
Imaging is selected based on clinical suspicion and risk stratification. The two main options are renal ultrasound and CT urography — covered in detail in Section 5 below.
Ultrasound is often the first-line imaging choice, particularly in lower-risk patients or where radiation exposure is a concern. CT urography is the gold standard for high-risk haematuria and provides the most comprehensive assessment of the entire urinary tract.
Cystoscopy — direct visualisation of the bladder lining — is a key part of the haematuria workup in most patients. It is the only investigation that can reliably detect bladder tumours, carcinoma in situ, and other mucosal abnormalities.
Flexible cystoscopy is performed under local anaesthetic in clinic. Rigid cystoscopy is performed under general or spinal anaesthetic and allows biopsy and treatment. Both are covered in detail in Section 6 below.
The pathway is always adapted to the individual. Not every patient needs every investigation.
Example — Mrs Evans, 65, smoker, visible haematuria:
History reveals two episodes of painless visible haematuria over three weeks. No dysuria. Ex-smoker, 30 pack-years. Urine MC&S: no infection. Blood tests: normal renal function. Risk stratification: high-risk (age, smoking, visible haematuria).
Pathway: CT urography + flexible cystoscopy arranged within 2 weeks. CT shows no upper tract abnormality. Cystoscopy reveals a 1.5cm papillary lesion on the posterior bladder wall. Referred for rigid cystoscopy and TURBT under general anaesthetic.
5. Imaging: Ultrasound and CT Urography
Imaging allows us to examine the kidneys, ureters, and bladder for structural abnormalities — tumours, stones, cysts, or obstruction. The choice of imaging depends on your risk profile, kidney function, and clinical findings.
Ultrasound vs CT Urography
Renal Ultrasound
A non-invasive, radiation-free scan using sound waves. Performed in two phases (full and post-void bladder). Excellent for detecting kidney cysts, hydronephrosis, and larger renal masses. Limitations: less sensitive for small tumours, ureteric lesions, and flat bladder lesions. Often used as first-line imaging in lower-risk patients or where radiation is a concern.
CT Urography (CTU)
The gold standard for haematuria investigation. A three-phase CT scan (non-contrast, nephrographic, and delayed/excretory phases) provides comprehensive assessment of the entire urinary tract. Requires normal kidney function (eGFR check essential before contrast). Contrast allergy history must be taken. Involves radiation exposure — MRI urography is an alternative where CT is contraindicated.
You will be asked to attend with a comfortably full bladder. A gel is applied to your abdomen and a handheld probe is moved across the skin. The scan is painless and takes approximately 20–30 minutes. A second set of images is taken after you have emptied your bladder (post-void residual measurement). Results are typically discussed at your follow-up appointment.
You will have a blood test to check kidney function before the scan. On the day, a cannula is placed in your arm for the contrast injection. The scan itself takes 10–20 minutes. You may feel a warm flush when the contrast is injected — this is normal. You will be asked to drink water and empty your bladder between phases.
If your kidney function is reduced, or if you have a contrast allergy, MRI urography may be arranged instead. The radiologist's report is reviewed at your follow-up appointment, where findings are explained and next steps agreed.
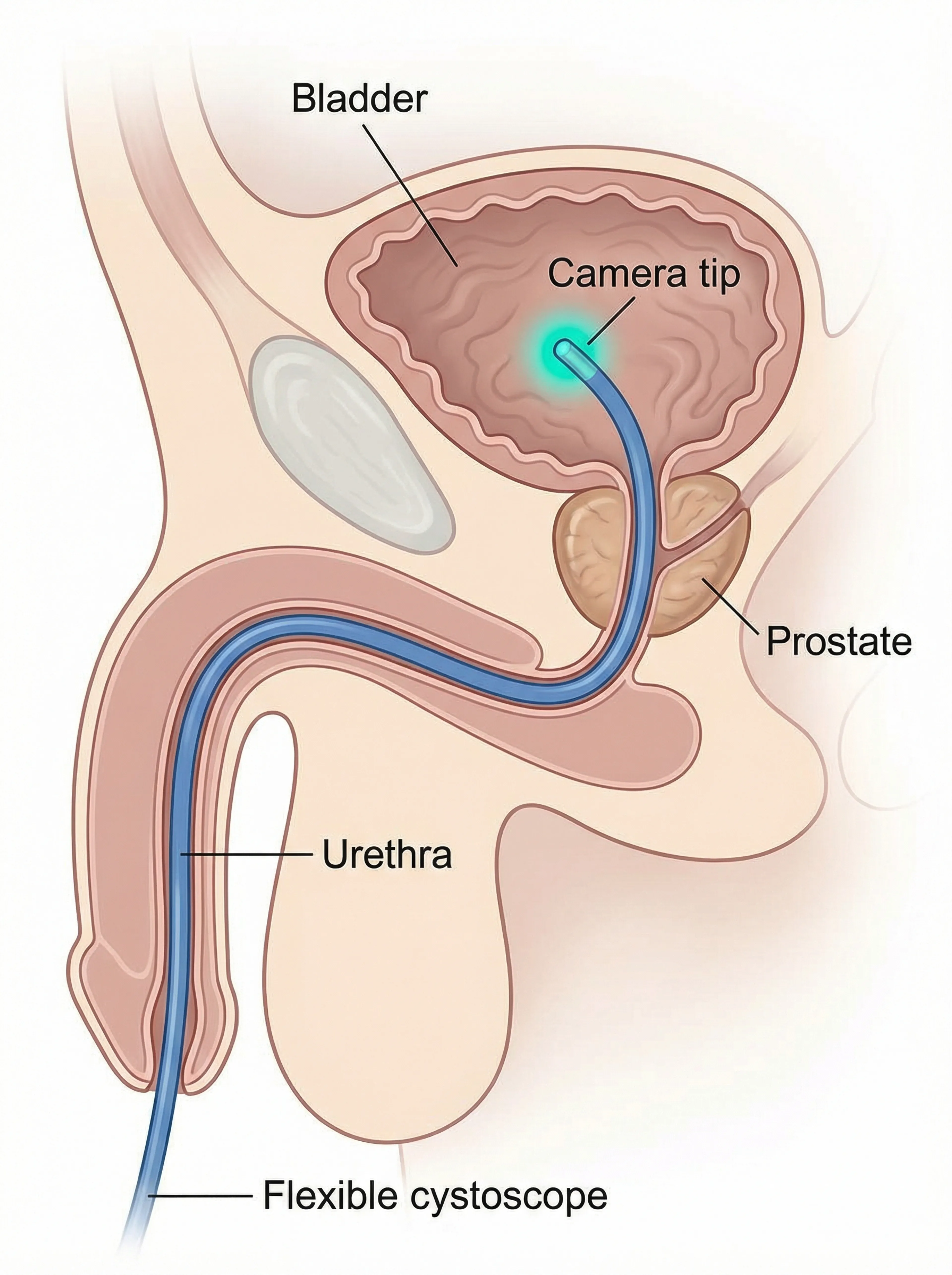
6. Cystoscopy
Cystoscopy is the direct visualisation of the inside of the bladder using a thin, flexible or rigid telescope. It is the most important investigation for detecting bladder pathology — including tumours, carcinoma in situ, and other mucosal abnormalities that imaging cannot reliably detect.
Flexible vs Rigid Cystoscopy
Flexible Cystoscopy
Performed under local anaesthetic gel in clinic. A thin, flexible telescope is passed through the urethra into the bladder. The procedure takes 5–10 minutes. You remain awake and can watch the screen. Used for diagnostic assessment — to look for tumours, inflammation, or other abnormalities. You can drive home afterwards.
Rigid Cystoscopy & TURBT
Performed under general or spinal anaesthetic in theatre. A rigid telescope allows biopsy of suspicious areas and resection of bladder tumours (TURBT — Transurethral Resection of Bladder Tumour). TURBT is both diagnostic (providing tissue for histology) and therapeutic (removing visible tumour). A urinary catheter is placed afterwards. See our surgical procedures hub for what to expect.
Local anaesthetic gel is instilled into the urethra and left for a few minutes. You will be positioned lying on your back. The flexible cystoscope is gently passed through the urethra — you may feel pressure or mild discomfort, but it should not be painful. The entire bladder lining is systematically inspected. The procedure takes 5–10 minutes.
Afterwards, you may experience mild burning on urination for 24–48 hours and a small amount of blood in the urine. Drinking plenty of water helps. You can drive home and return to normal activities the same day.
Rigid cystoscopy is performed under general or spinal anaesthetic. A rigid telescope is passed through the urethra, allowing biopsy of suspicious areas and resection of bladder tumours (TURBT). TURBT provides tissue for histological diagnosis and removes visible tumour in the same procedure.
A urinary catheter is placed at the end of the procedure and typically removed after 1–2 days. Hospital stay is usually 1–2 nights. Recovery varies depending on the extent of resection. See our surgical procedures hub for detailed recovery information.
Photodynamic Diagnosis (PDD / Blue Light Cystoscopy): A photosensitising agent is instilled into the bladder before the procedure. Under blue light, cancerous and pre-cancerous cells fluoresce pink/red, making them visible when they might be missed under standard white light. Particularly useful for detecting carcinoma in situ (CIS).
Narrow Band Imaging (NBI): Uses specific wavelengths of light to enhance the visibility of blood vessels in the bladder wall, improving detection of flat or subtle lesions.
These techniques are used selectively — your surgeon will advise if they are appropriate for your case.
7. When to Seek Urgent Medical Attention
Most haematuria does not require emergency attendance. However, certain situations demand immediate action. If any of the following apply, do not wait for a routine appointment.
Red Flags — Act Now
Visible Blood with Clots
Large clots can block the urethra and prevent urination (clot retention). This is a urological emergency. Go to A&E immediately.
Acute Urinary Retention
If you cannot pass urine at all, this is an emergency regardless of whether haematuria is present. Go to A&E immediately.
Signs of Kidney Infection
High fever, rigors (shaking chills), loin pain, and feeling very unwell alongside haematuria suggest pyelonephritis. This requires urgent assessment and IV antibiotics. Go to A&E or call 999.
Haematuria After Trauma
Blood in the urine following an accident, fall, or blunt abdominal or pelvic injury requires urgent assessment to exclude internal organ damage. Go to A&E immediately.
Feeling Very Unwell
Haematuria accompanied by severe pain, collapse, confusion, or feeling systemically very unwell requires emergency assessment. Call 999 or go to A&E.
Not Sure What to Do?
If you have visible haematuria but none of the red flags above, contact your GP for an urgent same-week appointment. If you are unsure, call NHS 111. For any of the red flags above: go to A&E or call 999.
8. What Happens After Diagnosis
Once investigations are complete, the findings are reviewed and a personalised management plan is agreed. The approach depends entirely on what has been found — and on your preferences, circumstances, and priorities.
After all investigations are complete, a follow-up appointment is arranged to discuss the findings in full. If a diagnosis has been reached, the management options are explained clearly — including what each option involves, its benefits and risks, and what to expect. If no cause has been found (idiopathic haematuria), a monitoring plan is agreed.
Examples of Management by Diagnosis
Urinary Tract Infection
A course of antibiotics targeted to the causative organism. Follow-up urine test to confirm clearance. If haematuria persists after treatment, further investigation is arranged.
Kidney or Bladder Stones
Small stones may pass spontaneously with hydration and analgesia. Larger stones may require ESWL (shockwave lithotripsy), ureteroscopy, or surgery. Management is discussed via our urinary problems hub.
BPH (Enlarged Prostate)
Lifestyle modifications, alpha-blockers, 5-alpha reductase inhibitors, or surgical options depending on severity. See our LUTS diagnosis guide and BPH surgery page for detail.
Bladder Cancer
Staging investigations followed by TURBT, intravesical therapy (BCG or chemotherapy), radical cystectomy, or radiotherapy depending on stage and grade. Surveillance cystoscopy is a key part of long-term management. Discussed via our treatment hub.
Kidney Tumour
Staging CT scan followed by partial or radical nephrectomy, ablation, or active surveillance depending on tumour size and characteristics. Discussed via our treatment hub.
Glomerular Disease
Nephrology referral for kidney biopsy, monitoring, blood pressure control, and immunosuppression where indicated. Management is led by the nephrology team.
Idiopathic Haematuria
No cause found despite thorough investigation. Reassurance is provided alongside a structured follow-up monitoring plan — typically annual urine tests and blood pressure checks. If haematuria recurs or new symptoms develop, re-investigation is arranged.
Every management decision is made collaboratively. At the follow-up appointment, the diagnosis is explained clearly, management options are discussed with their benefits and risks, your questions are answered, and a plan is agreed together. There is no single 'right' answer for every patient — the right plan is the one that fits your diagnosis, your circumstances, and your preferences.
This guide focuses on diagnosis, not treatment. Detailed information about specific treatments — for bladder cancer, kidney tumours, BPH, and other conditions — is available on dedicated condition and treatment pages. Use the links above or visit our treatment hub and urinary problems hub.
Frequently Asked Questions
No. The majority of haematuria cases are caused by benign conditions — UTIs, kidney stones, BPH, or exercise. However, because a proportion of cases do indicate serious pathology (including cancer), every episode requires investigation. The investigation is what tells us the cause — not the symptom itself.
Yes. A single episode of visible haematuria — even if it has not recurred — requires investigation. Bladder tumours, for example, can bleed intermittently. The absence of further episodes does not mean the cause has resolved.
A positive dipstick with a negative microscopy (no red blood cells seen) can occur with haemoglobinuria (haemoglobin in the urine without intact red cells) or myoglobinuria (from muscle breakdown). These have different causes and implications. Your clinician will interpret the results in the context of your full clinical picture.
Most patients describe flexible cystoscopy as uncomfortable rather than painful. Local anaesthetic gel is used, and the procedure takes only 5–10 minutes. The most common sensation is pressure as the scope passes through the urethra. Mild burning on urination for 24–48 hours afterwards is normal.
CT urography and cystoscopy assess different parts of the urinary tract. CT is excellent for the kidneys and ureters but cannot reliably detect small or flat bladder lesions. Cystoscopy directly visualises the bladder lining and can detect abnormalities that CT misses. Together, they provide a comprehensive assessment of the entire urinary tract.
Idiopathic haematuria — haematuria with no identifiable cause despite thorough investigation — is not uncommon, particularly in younger patients with microscopic haematuria. A structured monitoring plan is agreed: typically annual urine tests and blood pressure checks. If haematuria recurs, becomes visible, or new symptoms develop, re-investigation is arranged promptly.
References & Clinical Standards
This guide is informed by the following clinical guidelines and sources:
- NICE Guideline NG12 — Suspected cancer: recognition and referral (2015, updated 2023). Defines the 2-week-wait referral criteria for haematuria.
- EAU Guidelines on Non-Muscle-Invasive Bladder Cancer (European Association of Urology, 2024 edition).
- EAU Guidelines on Renal Cell Carcinoma (European Association of Urology, 2024 edition).
- EAU Guidelines on Upper Urinary Tract Urothelial Carcinoma (European Association of Urology, 2024 edition).
- SIGN Guideline 104 — Management of transitional cell carcinoma of the bladder (Scottish Intercollegiate Guidelines Network).
- British Association of Urological Surgeons (BAUS) — Patient information on haematuria, flexible cystoscopy, and TURBT.
- Kidney Disease: Improving Global Outcomes (KDIGO) — Clinical practice guidelines for glomerulonephritis.
- NHS England — 2-week wait referral guidance for urological cancers.
Important: This guide is for educational purposes only. It does not constitute medical advice and cannot replace a personal consultation with a qualified clinician. If you have concerns about blood in your urine, please seek medical assessment. This content has been reviewed in accordance with PIF TICK quality standards for health information.
My Approach to Haematuria
What You Can Expect
Systematic & Thorough
Every case of haematuria is investigated fully. Risk stratification guides the pace and extent of the workup — but no cause is assumed and no investigation is skipped without good reason.
Clear Communication
You will understand what each investigation involves, what we are looking for, and what the results mean. Nothing is left unexplained.
Efficiency & Urgency
Haematuria is time-sensitive. Same-week appointments are available. Where urgent referral is needed, it is arranged without delay.
Collaborative Decision-Making
Management decisions are made together. Your preferences, circumstances, and priorities shape the plan — not just the diagnosis.
Your Next Step
If you have noticed blood in your urine — even once, even if it has resolved — the right step is to get it assessed. Most causes are benign. But the only way to know is to investigate. Book an appointment and we will take it from there.
Ready to Get Answers?
Same-week appointments available. We'll assess your haematuria systematically, explain every step, and agree a plan together.